Universal Mask Mandates: Science, Politics, Health & Liability Concerns
POLITICS ASIDE, when is it reasonable to require health departments, public servants, employers and media to produce the SCIENCE to support mask mandates? Surely, there must be a plethora of studies that 100% prove healthy people being required to wear face masks daily, over extended hours, indoors/out and under any/every working condition constitutes a DO NO HARM measure (i.e. the baseline for medical practice, NOT malpractice).
What DOES the science say?
Alerts, Recalls & Scientific Guidance for public health decision-making…
NEWS: BOMBSHELL: Disposable blue face masks found to contain toxic, asbestos-like substance that destroys lungs (3/21/2021)
Cliff Notes & Pull Quotes:
Health Canada issued warning about blue and gray disposable masks containing asbestos-like substance associated with “early pulmonary toxicity.”
Their preliminary risk assessment raised concern that inhalation of microscopic grapheme particulates “could cause severe lung damage.”
CBC News noted Graphene “…can be harmful to lungs when inhaled and can cause long-term health problems.”
The feature states that some children in daycare settings felt “as though they were swallowing cat hair while wearing them.” AND “We now know…children were inhaling the equivalent of asbestos all day long.”
Used in classrooms across Canada, SNN200642 masks (made in China; distributed by Quebec-based Métallifer) “had never been tested for safety or effectiveness” AND “…never should have been used.”
People are being advised to “immediately stop using the masks.”
RELATED NEWS: Mask Recall -- Montreal transit workers wearing potentially toxic masks (3/29/2021)
Cliff Notes & Pull Quotes:
Mass recall now underway as Transit workers learn face masks they were supplied to wear for at least six months have now been identified as potentially toxic.
One spokesman stated that, “…at the time that we acquired the masks they were in compliance with the regulations.”
Masks recalled were imported from China.
Cited as “a potential emerging risk” were face masks “coated with nanoform grapheme materials” and it was noted that “Breathing in this substance presents an ‘unacceptable’ risk of toxicity to the lungs.”
Among those wearing problematic masks include teachers, daycare workers and health-care workers. The full list of affected has not yet been completed. Work to identify such groups/individuals is ongoing. It is known that “hundreds of thousands” have been used by transit employees.
Masks were purchased based on lowest bid (by Metallifer, on of the transit agency’s main suppliers). One unnamed mechanic said they were “given the masks to wear every day, 40 to 60 hours per week, since what he recalled as July or August 2020.”
RELATED NEWS: Mask Recall -- Potentially toxic masks distributed in schools and daycares in Quebec(3/26/2021)
Cliff Notes & Pull Quotes:
Health Canada warns of potential for “early pulmonary toxicity” from masks distributed to Quebec schools and daycares.
Recall of the grey and blue masks (SNN200442) is underway, as they could contain potentially toxic material dangerous to lungs.
Preliminary risk assessment indicates, “potential for early lung damage associated with inhalation of microscopic Graphene particles.” Graphene particles can be “harmful to lungs when inhaled and can cause long-term health problems.”
According to the article, “Some daycare educators had been suspicious of these grey and blue masks for a while because they felt like they were swallowing cat hair while wearing them.”
The article includes more details with regard to the recall that relates to local daycares and schools.
The masks were manufactured in China and distributed by Quebec-based distributor, Metallifer.
Expert Reviews & Commentaries…

EMPLOYER MUST WATCH -- VIDEO: The Science of Masks (with transcript and study links)
This comprehensive and clearly articulated video addresses the science of masks available. It is an absolute MUST WATCH/READ for anyone concerned about their health and/or potential for negative effects and/or liability (i.e. why this is marked as an “Employer Must Watch” item).
Transcript:
Today I’d like to share some of the science on this: a surgical mask and other face coverings.
Protective masks have been used in healthcare for many years. But how did all this begin? And how effective are they really?
Mask-wearing has been practiced for centuries by cultures all over the world, for ritual, celebration and even more. But some of the earliest examples of mask wearing in medicine appeared around the 1600s when physician, Charles de Lorme, created the earliest versions of a hazmat suit, featuring a waxed fabric overcoat, a lengthy cane to examine people without touching them and a menacing beaked mask that had a surprising intent behind its design. You see, medical professionals at the time believed in the Miasmatic cause of illness and disease transmission; or what they referred to as, “bad air.” So the enclosed beaked mask wasn’t to specifically defend against the “bad air;” it was used to inhale good air by stuffing the beak full of herbs and spices. The practitioner could now sniff the good air in the mask to crowd out the “bad air.”
You may think that this was a long time ago, but the Maismatic theory of “bad air” didn’t become obsolete until the 20th century. By this time, the germ theory of disease had fully taken hold and, by the early 1900’s, physicians were now beginning to wear preliminary versions of surgical masks, with a primary function of protecting the patient from contamination and surgical site infection. It eventually became common practice for health care workers to wear masks in the operating room. Though, as more hygienic practices have been incorporated into surgical rooms, several scientists have sought out to discover whether or not the ritual of wearing a mask in surgery had a high level of effectiveness in preventing infection.
Surprisingly, several studies, including a meta-analysis published in 2016, Cochrane Systematic Review, found that when physicians wore a mask or didn’t wear a mask, “there was no statistically significant difference in infection rates between the masked and unmasked group in any of the trials.” Even over a hundred years after the inception of the face mask in surgery, the researchers noted that, at best, “it is unclear whether wearing surgical face masks results in any harm or benefit to the patient undergoing clean surgery.”
Other studies published in the Journal of Hospital Infection and more, have also concluded that the use of surgical masks in surgery are obsolete and unnecessary. Researchers at the Center for Infectious Disease Research and Policy (CIDRAP) summarized it by stating, “Clinical trials in the surgery theater have found no difference in wound infection rates with and without surgical masks. Despite these findings, it has been difficult for surgeons to give up a long-standing practice.”
Surgical masks were developed to be used in surgery, yet have been found to be ineffective in their purpose to reduce rates of infection. But surgical masks have recently taken on a new role and are now being touted for their use and helping to reduce the spread of communicable infections within the general population.
So let’s take a look at how well surgical masks and other face coverings do in the presence of viruses, bacteria and other pathogens. It appears to be obvious that blocking one’s mouth and nose would prevent the spread of bacteria, viruses and other microbes. Yet, these microscopic entities don’t operate on the obvious. In fact, they operate in a way that defies surface-level logic altogether.
In reality, the actual size and capability of a bacteria and viruses just might shock you. Using the size of a human hair as a comparison, a single strand of hair is about 80 micrometers in thickness. to get to the size of a single bacterial cell, you have to divide the size of a hair by 40. A single bacterial cell is just to micrometers or 1/40th the width of a hair. Now, here’s where it gets really uncanny: a virus particle is too small to be measured in micrometers. It’s measured in nanometers. And at the size of about 17 to 140 nanometers, you can actually fit hundreds or even thousands of viruses into a single bacteria cell. These pathogens are inordinately small and the protective pore size of conventional cloth and surgical masks are gigantic compared to viruses. Virus particles could slip through as easily as flies going through a chain-link fence.
But the potential benefit of a mask is that viruses travel from our bodies via aerosols and droplets. Whether you are talking, shouting, sneezing, coughing or simply breathing, you are continuously omitting aerosols and droplets into the air. Think about how you can sometimes see your breath on a cold day. The change in humidity allows you to better see what is often invisible, but always happening. These tiny, sometimes invisible droplets contain an array of bacterial cells and viruses. And droplets typically measure between 5 and 10 micrometers in diameter; this is large enough to get caught by the filtering action of a conventional mask when you cough or exhale. And those that escape your mask would theoretically fall to the floor because of their density. But, the strange thing is that almost all droplets will evaporate before hitting the ground and free the virus particles within them to remain in the air longer (meaning that they can transmit disease through the airborne route, for anyone who walks into them).
Aerosols are what form when smaller droplets evaporate faster than they can fall to the ground. They play by different rules and can enable viruses to remain in the air for several minutes or even or even up to a couple of hours according to the CDC. The purpose of face masks is advocated to keep your microbes contained and protect other people from you.
According to the United States FDA, if worn properly, a surgical mask is meant to help block large particle droplets that may contain germs, keeping it from reaching your mouth and nose.
But, while a surgical mask may be effective in blocking large particle droplets, a face mask, by design, does not filter or block very small particles in the air that may be transmitted my coughs, sneezes or certain medical procedures. Surgical masks also do not provide complete protection from germs and other contaminants because of the loose fit between the surface of the mask and your face.
So, even though some of the larger particles can be trapped in the mask and reduce forward projection, with a special type of imaging technique, we can now see that when someone breathes, talks, sneezes or talks into a mask, the forward displacement of aerosols and droplets is reduced and instead, the microbes are dispersed above the mask, below the mask, out the sides and even through the mask itself, based on the material of the mask and how tightly it is sealed.
There is a range of protection, from makeshift cloth mask to medical mask, but this disbursement of virus particles is still occurring and this is what most people are not being educated about. It’s the fact that when we breathe, talk, cough or sneeze into a mask we are all still spreading millions of virus particles and bacteria into our environment.
And all it takes is just one virus particle to infect someone and set off a cascade of infectious disease. Again, viruses can remain in the air for a couple of minutes or even a couple of hours and data cited in the New England Journal of Medicine noted that aerosols from infected persons may pose an inhalation threat even at considerable distances and especially in enclosed spaces, particularly if there is poor ventilation.
So how does this data regarding masks and the behavior of viruses play out in the real world?
Well a randomized, peer-reviewed study published in the BMJ looked at the efficacy of masks to prevent viral infection in hospital healthcare workers in 15 different hospitals. The participants were randomized into three different groups. One group wore medical masks at all times on their work shift. A second group wore cloth masks at all times on their shift. And a third group, the control group, was allowed general practice which included occasionally wearing a mask or not wearing a mask at all.
Here’s what the study found: a percentage of healthcare workers in all groups contracted infections. But the participants wearing cloth masks had significantly higher rates of infections then the participants wearing surgical masks. In fact, healthcare workers wearing cloth masks were 13 times more likely to experience viral type infections than those wearing medical masks.
Now here’s what’s even more shocking about the study: not only were the rates of infections higher in the cloth mask wearing group than the medical mask group, the rates of infection in the cloth mask group were significantly higher than the people in the control group (who were allowed to occasionally wear a mask or not even wearing mask at all).
Please listen to that again.
This real-world setting, peer-reviewed study found that you are more likely to contract a viral infection by excessively wearing cloth mask then not strictly wearing a mask or wearing no mask at all. This is it’s not to say that a mask cannot be helpful in acute situations, but being advised to wear a cloth face mask could be outright dangerous.
The researchers found that the penetration of cloth masks by particles was almost 97% and medical masks, about 44%. The medical mask didn’t do particularly well. But the performance of the cloth mask we’re absolutely horrendous. The scientists in the study collected enough data to conclude that the wearing of a cloth mask can potentially increase your risk of getting sick.
But the question is, why?
The researchers stated that, “moisture retention and poor filtration may result in increased risk of infection with cloth masks and that cloth masks should not be recommended.”
The data shows that the cloth mask material actually creates a reservoir for pathogen growth; a wet, trapped environment where your own microbes as well as pathogens from the environment around you increasingly stick to the mask and colonize. Where, in the natural world, your droplets would be diluted into the air, you are, in essence, creating a wet microhabitat on your face that can make it even better at collecting other people’s microbes on it.
A 2015 study conducted by scientists at Oxford University found that, “The accumulation of moisture during prolonged usage may exacerbate this problem by increasing resistance to airflow. Moisture accumulation is also thought to facilitate the movement of contaminants through the material of the mask itself.”
Unfortunately, public health officials have repeatedly endorsed cloth masks to the public and these recommendations have led to an explosion in companies creating and selling cloth face masks. It may have been well-intentioned, but it was not based on valid science.
Now what may be even more unanticipated is that these effects are seen in other types of masks too. In fact, the study from Oxford revealing that moisture accumulation and air flow resistance can facilitate the movement of more microbes through the mask was actually done on surgical masks and the data shows that, the longer these and other types of masks are kept on, the more problems start to arise with their effectiveness.
A meta-analysis of 19 randomized controlled trials published in the International Journal of Nursing Studies examined the effectiveness of masks in reducing infections in 8 community settings, 6 healthcare settings and 5 as source control. The study concluded that, “Medical masks were not effective and cloth masks were even less effective.”
What’s even less effective than not effective? That means, in the real world, clinical evidence shows that they’re worthless and, at worst, potentially dangerous.
The confusing part for the public is that they see health organizations and news reports that actually recommend cloth masks even above medical masks, based off of unrealistic studies were people put on a mask for a minute, cough into a Petri dish and then take the mask off. Then the study is like, “See? These masks work great!” But that is not how things work in the real world.
This should all be a little bit alarming because all most people are hearing is to just wear something – anything helps! And this idea is based on very rudimentary beliefs about droplets and aerosols.
Yes, a mask can reduce the distance of them projecting forward but they’re not suddenly disappearing into a black hole when you cough or breathe into a mask.
They are spraying above the mask, below the mask, out of the sides and even through the mask as well. They are spreading all over your clothes, your face, your hair and even the environment around you.
To top it off, the moisture trap created by encasing your mouth and nose within the mask creates a reservoir for pathogen growth that encourages the movement of microbes through the mask itself.
Unfortunately, the push to get new data out to affirm the efficacy of these masks are extremely speculative and engendering a false sense of security in the mask abilities.
One of the most recent studies boasted the headline that, “Surgical masks can reduce spread of covid-19 virus by up to 75%.” But if you actually examine the data, you’d find the courageous participants tasked with simulating real life situations were… hamsters!
Hamsters were injected with covid-19 and placed in cages in plastic boxes next to another cage of uninfected hamsters. The cages were separated by a hole… Because, you know, they’re simulating human situations right?
In some parts of the study, they put a surgical mask between the hole. Other times, they didn’t. These were the conditions in which they came up with the 75% effectiveness figure.
The lead researcher in the study said, “In our hamster experiment, it shows very clearly that if infected hamsters or humans, especially asymptomatic were symptomatic ones, put on a mask, they actually protect other people.” How in the hamster can they say that this study shows anything “very clearly?”
The most troubling part is that countless people, including health professionals have referenced this study to claim the efficacy of masks to prevent viral infections while studies conducted in real world settings prove otherwise.
I should not have to say this, but this study wasn’t done in real-world conditions. And I should not have to stay that we are, in fact, not hamsters, isolated in cages, with a hole separating us from each other. But, at a time when so many people like to latch onto minutea and totally miss the bigger picture and the science, I have to say it blatantly.
Another recent study conducted by researchers at Texas A&M declared that face masks “prevented more than 66,000 infections in New York City in less than a month.” The lead researcher stated that, “By analyzing the pandemic trends without face covering, using the statistical method and by projecting the trend, we calculated that over 66,000 infections were prevented by using a face mask in a little over 1 month in New York City.”
Yet again, if you read into the study, it’s a study affirming how droplets and aerosols travel, which we already know, and not a study on mask effectiveness. The claims that the masks prevented 66,000 infections are based on hasty assumptions of universal consistency in mask quality, mask fit, duration of time worn, assumption that the wearers aren’t touching their face, that their aerosols and droplets aren’t being deflected and sprayed all over their face, hair, clothes and creating clouds of droplets from above, below been through the sides of the mask and it’s also assuming that the masks are effective in the first place, which the vast majority of real-world, clinical trials we’ve covered already show that they’re not.
Their gross estimates also fail to differentiate the effects that shelter in place and social distancing mandates had, verse is wearing a mask in public. In fact, the infection rates were already trending down when the stay-at-home mandates were in place and this study suddenly gives unsubstantiated credit to face masks.
The assumption of universal conditions is not how science works. And it’s not how viruses work in the real world.
The lead researcher in the study stated that, “our work also highlights that sound science is essential in decision-making for the current and future public health pandemics.” if this is sound science, we are all going to need to get her ears checked. Because herein lies the problem: in the real world, inaccurate, speculative research like this is determining decision-making for the current and future public health issues. There are more holes in their theories that a fresh pair of Crocs! Yet, once it’s embedded into the minds of the public, false assumptions and bad science begin to spread like wildfire.
Now let’s look at the effectiveness of the most prestigious type of mask and how it stacks up against the surgical mask. Remembering that virus particles generally range from 17 to 140 nanometers, the American Chemical Society has noted that the N95 mask filters about 85% of particles smaller than 300 nanometers. Yes, most viruses are much smaller than that and no, it’s not always effective but, going back to our science on aerosols and droplets, it’s likely doing a better job at reducing viral spread then other masks, at least.
But, let’s take a look at the boots on the ground data. A 2017 study conducted by Chinese researchers found that targeted, intermittent use of N95 respirators while doing high-risk procedures or caring for patients with known respiratory illness actually caused higher rates of viral infections in healthcare workers (wearing the N95 masks) then those wearing surgical masks. And even more surprising is that participants wearing the N95 masks had higher rates of infections than the control group who are not required to wear either mask at all.
Wait, what? N95 respirators are supposed to be the gold standard. How on earth can they be out performed by casual wearing or not wearing of masks seen in the control group?
That didn’t look too good on paper for the researchers, so they had another group who had to constantly wear the N95 mask (for their entire shift) and, lo and behold, it did outperform the surgical mask and control group. The researchers now found a lower rate of droplet related infections, however, the protection from confirmed influenza virus was not sticking its statistically significant.
We could reasonably say that there’s mixed results here. So let’s take a look at some of the other studies.
In a randomized controlled trial at 446 nurses emergency departments, medical units and pediatric units, approximately half of the nurses were assigned to wear a surgical mask and the other half were assigned to wear a fit tested, N95 respirator, to study their effectiveness against the influenza virus. The two and a half months study published in the Journal of the American Medical Association revealed that 23. 6% of the nurses in the surgical mask group contracted the virus, while 22. 5% of the n95 mask group contracted the virus. The effectiveness was almost identical…still not faring too well for the highly touted N95 mask, so let’s look at more.
In a meta-analysis published in the Canadian Medical Association Journal that included 6 clinical studies and 23 surrogate exposure studies, the scientists found no significant difference between the N95 respirators and surgical masks in associated risk of laboratory-confirmed respiratory infection or influenza-like illness.
These are real world examples of how effective these masks actually are – not speculating; not making gross assumptions.
This is how things work in reality. Even the very best mask doesn’t consistently outperform the most useless mask because the entire premise of a mask is ignoring the nature of how pathogens actually spread throughout the environment.
If this isn’t alarming enough, there’s another major issue that you need to know about. In the study that actually found some benefit in the N95 mask vs surgical mask, the healthcare workers we’re not allowed to take them off for their entire shift. But the data shows that, as with cloth masks, the longer they’re kept on the more problems start to arise.
A peer-reviewed study published in 2004 fitted patients with N95 masks and monitored the physiological impact the masks had on their bodies. 70% of the patients showed a significant reduction in partial pressure of oxygen. Partial pressure of oxygen (PAO2) reflect how well oxygen is able to move from the lungs to the blood and it is usually altered by severe illnesses. But in this case, it’s being reduced by suffocating one’s face with a mask. It’s dangerous and a major component of hypoxemic respiratory failure. And we can no longer overlook that this is happening.
Being that the N95 mask comes with substantial risk, researchers decided to look at the respiratory consequences of the N95 mask on pregnant, expecting mothers. The controlled clinical study published in the journal, Antimicrobial Resistance and Infection Control, recruited pregnant healthcare workers to wear N95 masks while doing just low-intensity activity and the results were shocking. Wearing the N95 mask reduce their normal volume of air displaced by inhalation and exhalation by 23%. The volume of gas inhaled or exhaled specifically from their lungs each minute was reduced by 25. 8% their volume of overall oxygen consumption was reduced by 13. 8%. And the ability to expire carbon dioxide was reduced by 17. 7%.
You may think that these effects were due to wearing the mask for an extended amount of time, but they were engaged in low-intensity activity for just 15 minutes!
The only reason that this was discovered is because someone saw pregnant mothers covering their breathing pathways with a mask and asked whether this practice could be dangerous for the mother and the baby.
But the truth is, this danger is occurring for all of us when we cover our breathing pathways. But someone had to have the courage to ask the question.
Unfortunately, there are websites that claim to “debunk” that wearing a mask could cause oxygen deficiency. Even sites run by major health organizations. But, their fact-checking seems to be scarce and even negligent in actually reviewing the facts.
The data has been out there all along – right at our fingertips – if we care to look at it; if our public health officials care to look at it. If our politicians care to look at it. But, it seems that the ability to analyze and respect scientific data has been replaced by bandwagoning and agendas that a no way serve the public except to immerse them in more fear, encourage agoraphobia and instill a false sense of security in something that is not only proven to be ineffective but is actually outright dangerous to our health.
Another thing that’s said to be “debunked” is that wearing a mask will cause carbon dioxide re-breathing. Yet, a peer-reviewed study published in the journal Anesthesia, revealed that within just 20 minutes of wearing a mask, the mean end-tidal carbon dioxide levels jumped up 13%. The researchers reported that, “The rise in end-tidal carbon dioxide is due to re-breathing of expired alveolar gas that is ‘trapped’ in the respirator.” They also noted that, “levels of end-tidal carbon dioxide have also been shown to significantly impair cognitive and psychomotor performance.”
This means that, in the real world setting, you now become a greater risk to yourself and others.
Another study published in the journal Ergonomics found that even at low work rates, wearing the mask contributed to significantly higher levels of CO2 re-breathing. With notable side effects such as fatigue, dizziness, headaches and muscular weakness, and just focusing on one of those side effects being headaches, when mandated to wear N95 masks, a peer-reviewed study published in 2006 found that almost 40% of healthcare workers developed face mask associated headaches.
It’s critical for us to realize that these reduced levels of oxygen can damage your lungs, your heart, and even damage your brain. And these dangerous effects aren’t just seen in N95 masks either.
Another peer-reviewed study published in 2008 reported surgical-mask-induced deoxygenation in physicians in surgery, while another study conducted by the CDC and published in the Annals of Work Exposures and Health revealed that by wearing a mask, the highly thermo-sensitive nature of the face and breathing pathways can be inhibited, leading to increased anxiety, elevated stress hormones, false suffocation alarm in the central nervous system and panic attacks.
What’s clear is that within minutes of putting on a mask, dangerous effects begin to set in, whether you realize it consciously or not. And the longer masks are worn, the more devastating their effects can be.
What’s particularly alarming is that many schools are beginning to mandate children to wear masks for hours a day, in order to be accepted back into the classroom. Keeping in mind that the benefits of masks are largely disproven and superficial, why on earth would we allow a society in which we put our children in harm’s way, by restricting their breathing for hours a day, just to be able to get an education?
The very heart of science is having the capacity to check your emotions and biases at the door and look at the data objectively – not just the data that supports your belief – and especially not the data that has been emotionalized and politicized.
I understand that the clinical evidence demonstrated here is not going to fit within the trending narrative. And with so much energy invested into making mask usage appear to be effective and ethical, many health professionals, public figures and politicians will find it difficult to admit that they made a mistake and finally shift the conversation to actually getting our citizens healthier, in clinically proven ways. But that’s okay. It doesn’t make the science any less real.
And that’s the thing about science: it doesn’t care what you believe.
Unfortunately, you can’t believe your way into making masks more effective than they are. And you can’t believe your way into masks not being utterly destructive to the health of ourselves and our children.
And this isn’t just a physical health issue. This is a mental health issue as well. What does seeing someone in a mask represent in our minds? A new study published in the Journal of Neuroscience affirmed how the brain immediately seeks out facial data to determine how trustworthy someone is and, accordingly, how safe or threatened you should feel. The researchers noted that our brains are specialized for recognizing faces. We are identifying each other by our faces and make instantaneous judgments about people. A person’s face provides a wealth of information. Within seconds of seeing a face, we immediately know much about a person including their gender, age, ethnicity, level of physical abilities, cues of sickness and disease, emotional state and more. This data enables us to make informed decisions on how we should interact or not interact with a person.
So why are masks so concerning for our mental health?
It’s because suddenly, this innate human instinct to assess someone’s face is shut off. In psychology, it has to do with the fear of the unknown. For most of us, seeing someone in a mask is associated with danger. We’re talking about hundreds of thousands of years of evolution being suppressed. To our brains, if someone is approaching you and you cannot see their face, they pose an immediate threat. You can consciously try to tell yourself they’re not a threat, but we can’t take evolution and easily turn it off. Not being able to recognize who’s behind a mask and what their intentions are is an automatic trigger for our sympathetic fight or flight system. Now, suddenly, we’re unable to do one of the things that makes us human. And many people are being driven into doing this indefinitely. It’s not based on science, but based on fear.
In developing children, this is an absolutely critical time for them to be able to see and read the faces of their peers as part of their mental and social development. Researchers have already noted a rise in childhood mental health issues resulting from the social lockdown, and noted that, “The full toll of covid-19 on children’s mental health won’t be known for years.”
It’s up to us to help put an end to these problems because, as of now, data published in the Canadian Medical Association Journal has already demonstrated massive increases in childhood stress disorders and depression caused by such dramatic changes in their daily social interactions.
Now going back to how simply seeing someone in a mask activates are fight or flight nervous system, this dangerous issue is further compounded by the act of covering our own faces as well. A study published in the International Archives of Occupational and Environmental Health found that there is a microclimate created within the mask that causes high breathing resistance, making it difficult for test subjects to breathe and take insufficient oxygen. This shortage of oxygen hyper stimulates the sympathetic fight or flight nervous system.
Another mask-related health problem fact-checking reports have presumably “debunked” is that wearing a mask doesn’t negatively affect your immune system. But, yet again, these reports fail to look at the facts regarding very basic human physiology. Scientists at the University of Edinburgh found that immune cells become overactive when oxygen levels are deranged and they “respond excessively to infection in a harmful way.”
A study published in the Journal of Evolutionary Biology found that hyperactivity of the fight or flight nervous system does increase immune gene expression but it does not increase in a way that helps to fight infection.
The scientist noted that abnormal stress (like what’s caused by self suffocation by a mask) is not an adaptive immune response. A short burst of inhibited breathing we’ll have a nominal impact on your immune system but, the longer a mask is obstructing your breathing, the more abnormal levels of stress hormones are produced and the more this activity becomes immunosuppressive, according to a study published in Integrative and Comparative Biology.
At this point, you’re probably wondering, “How do ideas like mandated mask-wearing catch on, even though their inordinately false and damaging to the public’s health?”
Well, part of it is the status quo – the idea that, “This is what we’ve always done.” As we discussed earlier, face masks have been used in medicine for several decades, even though they have been repeatedly proven to be ineffective. It’s become integrated into the culture.
As we shared at the beginning of this video, researchers at the Center for Infectious Disease Research & Policy summarized it by saying that, “Clinical trials in the surgery theater have found no difference in wound infection rates with and without surgical masks.” Despite these findings, it has been difficult for surgeons to give up the long-standing practice.
If the trusted authorities believe a thing that’s untrue, the public has almost no chance to believe otherwise. Some people think, “Of course masks work! Why do you think doctors wear them?” When in reality, it’s based on ritual and not on science.
Another reason false ideas catch on is that rituals tend to create cognitive biases.
A cognitive bias is a systematic tendency that leads our thinking away from a rational judgment. Even when presented with proof that what we believe is true is not actually true, we become so ingrained in our beliefs that anything that doesn’t fit our model of perception is often belittled, fought against, or ignored altogether. Our minds tend to work like a puzzle… if we come in contact with a new piece of data that fits, we add it to the puzzle. If the data doesn’t fit, we tend to discard it and throw it away. This puzzle picture we’re creating works at lightning speed, and we normally don’t realize it’s happening.
In the case of something highly emotional eyes like mask-wearing, something called a self-serving bias gets ramped up a thousand times higher.
A self-serving bias is a tendency to focus only on information that enhances the belief that we are right and rejects any information that we believe is incorrect. If a very smart person develops a self-serving bias for something that’s not true, they can become world-class at teaching and defending something that’s not true.
Our minds are always looking for things to affirm that we are right. So we actually have to proactively fight against this tendency because it can lead to dangerous selective perception and make our minds miss all of the contradictory information that can be incredibly valuable for us. In order to see all of the data and come to a more accurate conclusion, I have to come into the research knowing that I have a cognitive bias and no actively look for data that proves me wrong. It’s not always a comfortable thing to do, but it’s necessary to have a well-thought-out rational judgment. Especially in times of high emotion, it’s more important the number to develop this skill. If you’re willing to be wrong, you’ll be able to learn things that are outside of your biases. This will help you to make more effective decisions based on logic and not on fear.
Another reason that false ideas catch on is that cognitive biases are contagious.
The need to fit in and be accepted is a basic human instinct. According to an analysis in Frontiers in Psychology, the social aspects of the human brain are always working to negotiate and navigate social environments. And when you’re placed into a social construct – whether you were born into it are you buying to it – it creates the foundation for groupthink to occur.
Groupthink is a psychological phenomenon that manifest within a group of people where the desire for harmony or conformity in the group results and irrational or dysfunctional decision-making.
Right or wrong, you catch the belief from the group and it deeply affects your thinking. The groupthink becomes the unconscious driving force and ideas to support the groupthink are spread. For example, even though the data shows that wearing a mask is ineffective and even dangerous, catch phrases like, “it’s an act of love” – “it’s just a small sacrifice” – “it’s not about you” – and “stop being selfish,” are spread to affirm the belief of the group. It doesn’t matter that it’s irrational. The cognitive bias of the group makes it incredibly difficult to think otherwise.
And it’s not that statements like these are made with mal intent.
In fact, they can be made with great empathy and desire to help the cause. But when the beliefs are born out of a self-destructive cognitive bias, it can easily take on a life of its own and breed irrational behavior.
Again, this happens with very intelligent people all of the time. Let’s take a look at researchers from Harvard University for example. They recently published a report recommending that you should probably be wearing a mask to protect yourself during sexual situations right now. These researchers aren’t just being strangely freaky. They really believe that they are helping the cause. And guess what? That advice is going to leave countless people to wear protection downstairs and upstairs, as well. Not based on logic but based on the influence of the group think.
And with the spreading of irrational ideas, there’s an additional phenomenon that occurs today more than ever.
With the groupthink extending to celebrities and influencers, the power of celebrity politics is even more intrusive today. Celebrity politics is the act of a prominent person using their fame as a platform to influence others on ideology. Whether that ideology is wrong or not, other people tend to be more influenced by celebrities because narratives often persuade more than actual data.
So when your favorite celebrity issues a mask challenge to encourage more celebrities and the public to wear their mask, it creates a tidal wave bandwagoning behavior. One celebrity posted, “We know wearing a mask and make it hard for you to breathe. But, it’s more about protection than comfort.”
But not being able to breathe normally is not an issue of comfort. The discomfort of covering your face is your body telling you that this is wrong and dangerous. But cognitive biases, groupthink and celebrity politics can kick your logic right out of the window.
There are other reasons why false ideas catch on and have to do with ulterior motives, fear, passivity and more. Even many health professionals with good intentions have already accepted the prevailing beliefs regarding viruses and the effectiveness of masks. And their unconscious cognitive biases have them looking only for evidence to support their belief.
It takes a huge amount of courage to look at the evidence that proves you’re wrong, especially when you’ve publicly shown your belief in the wrong thing.
It takes a huge amount of courage to say, “You know what? I didn’t do my due diligence and examine the data. I didn’t look at all sides of this. I was wrong. I’m sorry. Now, let’s talk about how we can make this right.” We may think we’ve come a long way since the theory of Miasmatic illnesses or “bad air” being the cause of disease, yet today, millions of people are being told a very archaic belief that you must suffocate yourself in order to save yourself.
The science clearly disproves the effectiveness of masks, especially for the general population.
And by now you might be wondering,” What else is being misrepresented or ignored in the messaging to the public? And what can we actually do to protect ourselves and our families?” So let’s shift gears for a moment and talk about what really works to protect the health and well-being of our citizens, based on real clinical evidence.
Now, what I’m about to share might be a little bit staggering, but there are massive pandemics every single year that most people don’t know about. For example, the World Health Organization reported that upwards of 650,000 people die every single year from a specific infectious virus and it’s not the coronavirus. It’s influenza – the same influenza that most of us see as not a big issue; the same influenza virus that conventional medicine keeps making drugs for; up to 650, 000 people’s lives are lost from it, not just in a single year, but every year.
And that’s only counting the deaths related to the respiratory effects of influenza; and not even including the deaths from influenza-related seizures, organ failure and more, which would add tens of thousands more deaths on top of that. Thousands of people who take the supposed flu prevention drugs every single year still die. And the truth is, conventional medicine hasn’t remotely figured this thing out – there’s something that’s been around killing millions of people for decades.
Why on earth would we logically believe but covid-19 will be any different? That, in a few years, we’ll have a drug to protect us?
A cognitive bias might tell us that it’s different because the flu is tricky, it mutates. It keeps mutating every year but peer-reviewed data in the journal Cell stated that covid-19 has already mutated repeatedly and it will continue to do so because that’s what viruses do. That’s how science works but we still keep taking illogical approaches instead of paying attention to the data staring right in our faces.
Do you want to know the connecting factor between the majority of people who succumb to influenza and the people who succumb to covid-19? The vast majority of people who experience severe symptoms or even pass away from either of these infectious diseases have one or more pre-existing chronic illnesses. Some of the most recent data we have shows that nearly 90% of the patients who passed away with covid-19 in New York City had at least one pre-existing chronic disease. This means their pre-existing disease and Covid are comorbidities.
A comorbidity means there are multiple illnesses that may be the cause of, or strongly related to the cause of death. A study published in the Journal of the American Medical Association analyzes the data of covid-19 patients in New York City and uncovered that the most common comorbidities we’re hypertension, diabetes and obesity. Even though politicians and the sensationalized media make people believe that this virus is indiscriminately taking people’s lives, the truth is that approximately 9 out of 10 people who pass away with covid-19 already had a chronic disease that pre-subjected them to an abnormal immune response.
Why does this not raise a huge alarm for us?
Effective science doesn’t look at data and say, “We just need to put superficial masks on people with chronic illnesses and wait for a couple of years to give them a drug that will save them.” No! Effective science says, “Clearly, the most susceptible people are those with chronic illnesses. Let’s help them actually to improve or even eliminate those chronic illnesses. Let’s get to work right now to get our citizens healthier.
Obesity, heart disease and type 2 diabetes are the leading issues that make our citizens more susceptible to a viral infection.
Fixing these things and truly helping people with facts, not fear, brings up another inconvenient truth that was recently published in the Journal of American Medical Association. A 2018 peer-reviewed study found that poor diets are the #1 cause of poor health in the United States. Most of our countries chronic diseases are preventable and even reversible. The data shows that our food is the biggest issue and this is something that we can fix.
Do you really want to know why America was hit so hard by covid-19? America is arguably the sickest and most vulnerable industrialized nation in the world. According to a recent CIA report, America has the highest rate of obesity of any nation, with more than 40 million people. Right now, the United States has almost 200 million people who are either overweight or obese. And we have almost 125 million people who have lifestyle-related diabetes or pre-diabetes. We can’t keep pretending this underlying problem doesn’t exist. And we can’t keep on pretending that this is something we can’t fix. Instead of addressing what’s truly our greatest health epidemic, the thing that takes millions of lives prematurely every year, and the thing that makes are citizens more susceptible to all infectious diseases that go around and will continue to go around, instead of finally addressing these issues with intelligence, people deflect and use other cognitive biases.
“Well we can’t just get people healthy overnight, and we definitely can’t improve their immune system overnight…” Yet again, the data shows that this belief is unequivocally untrue. You absolutely can improve someone’s immune function and quickly. And you can absolutely demolish their immune function just as fast.
If we look at the immune response of the millions of people who contracted Covid-19 and had mild symptoms or no symptoms at all, it wasn’t a mask or a magic drug that did the job. It was their immune system. It simply did the job that it has evolved to do. Our immune system has an array of very dynamic, highly intelligent weapons at its disposal, including cytotoxic T cells, interferons, B cells and more.
But what is of special significance against the coronavirus are our NK cells, also known as are natural killer cells.
Our natural killer cells are so effective at killing coronavirus-infected cells that many pharmaceutical companies are scrambling to create vaccines that specifically manipulate your NK cells as a cure for covid-19. In fact, the FDA has already cleared an experimental drug for natural killer cell-based covid-19 therapy. But as usual, our conventional system that allows millions of people to die from preventable illnesses, every year, is looking at things through the lens of disease and pharmacology, and not through the lens of what actually makes people healthy.
We can improve the performance and production of natural killer cells and people who are susceptible starting now! We don’t have to wait!
However, the conflict of interest is that it’s generally free and accessible for everyone to do. A study conducted at Appalachian State University found that’s simply going for a short walk causes boosts in immune parameters most notably for your natural killer cell blood counts.
And data published in the journal Psychoneuroendocrinology found that sleep deprivation directly reduces the production and performance of your natural killer cells. Getting good sleep is more important than ever right now. But how many times have you seen anyone on major media tell you that?
Yet another study, this one published in the peer-reviewed journal Stress & Health found a significant correlation between the capacity of individuals to cope with daily life stress and they’re NK cell activity. Folks who don’t cope well with stress have significantly lower natural killer cell activity. How has most people’s stress management been through this experience? You already know the answer to that. And of course it’s been terrible. All we’re being fed when we look at major media and social media are reports reaffirming that there’s nothing you can do about this but suffocate yourself with a mask and hide out at home. The truth is, you need to look at the basic laws of physiology more than ever right now.
Your immune system needs oxygen to thrive.
Yet, for those who even have the courage to go outside in the open air, they’re wrapping their faces in material that obstructs they’re breathing – not because of science and logic, but because of fear. A study published in the BMJ demonstrated that the fear of covid-19 transmission in an open-air environment is illogical. You are almost 19 times less likely to contract the virus outside than by staying indoors.
Scientists at the International Laboratory for Air Quality in Health at Queensland University of Technology stated that, “Outdoors is safe and there’s certainly no cloud of virus-laden droplets hanging around. Firstly, any effects of droplets exhaled outside with you quickly diluted in outdoor air. So their concentrations would quickly become insignificant. In addition, the stability of the virus outside is significantly shorter than inside. So going outside is not a problem. It’s safe to go for a walk and jog and not worry about the virus in the air.”
Going outside in the fresh air with a mask on is like, well, going outside in the fresh air with a mask on. It’s not one of the shining moments of human advancement. But we can smarten up right now and stop acting like aliens on our own planet.
Your immune system also needs the right nutrition to thrive.
Your immune system, the thing that actually kills coronavirus, influenza and every other pathogen that you come in contact with, guess what it’s made of? It’s made of the food that you eat. Every cell in your body, including your immune cells, [is] literally made from the food that you eat and the water that you drink. Yet, you’d be hard-pressed to find an immunologist who is well educated on nutrition. Even though food is literally what makes your immune system, but that goes for every other field in conventional medicine. Being that your heart is made out of the food that you eat, you think that cardiologists receive a sufficient education in nutrition. But they hardly receive any at all. Can you start to see what’s wrong with this picture and why heart disease is the #1 killer in this country every single year?
Right now, make sure to eat plenty of real food and make sure to get in an array of micronutrients and omega-3 fatty acids. A study published in the Journal of Leukocyte Biology found omega threes appear to enhance the function of humeral immune cells that are responsible for your body remembering a virus and building up a long-term resistance to it.
Your immune system also needs sleep to thrive.
During sleep, your immune system works to replenish immune cells and repair your immune related organs. Research conducted by scientists at the Mayo Clinic found that people who don’t get quality sleep or get enough sleep are far more likely to get sick after being exposed to a virus. Even though the vast majority of people who experienced severe symptoms or even lost their life with covid-19 infections had one or more pre-existing chronic diseases.
Another common deflection point is that perfectly healthy people die from it too. Unfortunately, this is true. But [the way] we look at it disempowers us. First, it causes us to justify the deaths of the other 90% of people who weren’t “perfectly healthy.” It’s like 18 people with chronic diseases are drowning and two people without chronic disease is drown along with them. When their lives are lost we say, “Two of those people were perfectly healthy.” But in reality, all 20 could have been saved if we were doing the right thing to help them. Second, it doesn’t matter how healthy someone appears to be. If you’re sleep deprived, nutrient deficient or excessively stressed, any of these things can increase your incidence of infection, increase the duration of illness and increase the severity of illness as well.
None of us are immune from the basic laws of human physiology. For example, though it seems invisible, excess stress can be absolutely devastating to your immune system. Data reported in the Journal of the American Medical Association Internal Medicine reported that upwards of 80% of physician visits are for stress-related illnesses. While, in another study published by the American Academy of Sleep Medicine, researchers affirmed that just one night of sleep deprivation can deranged the immune system and increase your likelihood of infection.
We have basic human needs that must be met.
And this is our opportunity to help our communities get educated to effectively meet them. What if every message to wear a mask was replaced with, or even coupled with, advice from health officials to help to reduce stress, why stress management is essential in reducing your risk of infection and provide some clinically proven stress management practices for everyone. What if every message to wear a mask was coupled with advice from health officials to make sure you’re getting enough sleep right now, why sleep is essential and reducing your risk of serious infection and provide some simple, actionable steps that people can use to make it happen.
With the motivation people have had to stay safe, we could have revolutionized our society by now. But that’s not what we did. And that’s why it’s up to us to make this message go viral.
When we hear a story about the origins like the beak medical mask, we tend to think that it was so primitive that we all have it figured out now. But every single day we have new discoveries in science that have overturned long-held beliefs that were simply not true, unsubstantiated and even outright dangerous.
Arthur Schopenhauer stated that, “All truth passes through three stages. First, it is ridiculed. Second, it is violently opposed. Third, it is accepted as being self-evident.” We need to transition through these phases quickly now. Because millions of lives depend on it. Our children’s lives depend on it. And our future depends on it.
The next infectious disease is right around the corner; and the next; and the next one after that. Despite rapid advancements in medical science, our immune system is still the main weapon against infections and, if we don’t fix the culture that’s damaging our immune system, we will continue to lose lives unnecessarily.
The beauty of science is to be able to ask questions, to think for multiple perspectives and to come to well fought out conclusions for ourselves.
It’s time to put facts over fear and to help our families and our communities to get healthier. We can no longer allow ourselves to be divided. We can no longer allow ourselves to abandon reason in the face of uncertainty. And we can no longer allow ourselves to abandon our humanity in the face of fear. It’s time to implement real solutions for our citizens. It’s time to change our world for the better.
SCIENTIFIC REVIEW: Face masks, lies, damn lies, and public health officials: "A growing body of evidence" (August 2020)
Cliff Notes & Pull Quotes:
This item by D.G. Rancourt (Ontario Civil Liberties Association) is related to two others, as follows:
1) a white paper titled “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy.”
2) a follow-up (as previous promised to publish any contrary evidence) feature titled, “Still No Conclusive Evidence Justifying Mandatory Masks.”
This feature opens with the following abstract:
“A vile new mantra is on the lips of every public health official and politician in the global campaign to force universal masking on the general public: “there is a growing body of evidence”. This propagandistic phrase is a vector designed to achieve five main goals: – Give the false impression that a balance of evidence now proves that masks reduce the transmission of COVID-19 – Falsely assimilate commentary made in scientific venues with “evidence” – Hide the fact that a decade’s worth of policy-grade evidence proves the opposite: that masks are ineffective with viral respiratory diseases – Hide the fact that there is now direct observational proof that cloth masks do not prevent exhalation of clouds of suspended aerosol particles; above, below and through the masks – Deter attention away from the considerable known harms and risks due to face masks, applied to entire populations The said harms and risks include that a cloth mask becomes a culture medium for a large variety of bacterial pathogens, and a collector of viral pathogens; given the hot and humid environment and the constant source, where home fabrics are hydrophilic whereas medical masks are hydrophobic. In short, I argue: op-eds are not “evidence”, irrelevance does not help, and more bias does not remove bias. Their mantra of “a growing body of evidence” is a self-serving contrivance that impedes good science and threatens public safety. I prove that there is no policy-grade evidence to support forced masking on the general population, and that all the latest-decade’s policy-grade evidence points to the opposite: NOT recommending forced masking of the general population. Therefore, the politicians and health authorities are acting without legitimacy and recklessly.”
SWISS POLICY RESEARCH: Are Face Masks Effective? The evidence (9/28/2020)
Cliff Notes & Pull Quotes:
This document presents:
1) Studies on the effectiveness of face masks includes sections on “Additional aspects” and “Development of cases after mask mandates”
2) Studies claiming face masks are effective
3) Risks Associated with face masks
RE: Studies on effectiveness
1) 10 studies/reviews from around the world are presented
— general conclusion: “So far, most studies found little to no evidence for the effectiveness of cloth face masks in the general population, neither as personal protective equipment nor as a source control.”
— Results include:
1) “face masks had no effect, neither as personal protective equipment nor as a source control”
2) “no evidence for the effectiveness of cloth masks against virus infection or transmission”
3) “mask requirement was of no benefit and could even increase the risk of infection”
4) “face masks have no effect in everyday life, neither as self-protection nor to protect third parties”
5) “cloth face masks offer little to no protection in everyday life”
6) “face masks didn’t reduce influenza-like illness (ILI) cases, neither in the general population nor in health care workers”
7) “…evidence is not sufficiently strong to support widespread use of facemasks…”
8) “cloth masks ‘offer zero protection against coronavirus’ due to their large pore size and generally poor fit”
9) “cloth masks were penetrated by 97% of particles and may increase infection risk by retaining moisture or repeated use”
10) “no evidence for the effectiveness of cloth face masks and the improper daily use of masks by the public may in fact lead to numerous additional infections”
— Additional aspects:
1) increasing evidence of transmission via smaller aerosols (not just droplets), rendering cloth masks ineffective (“90% of aerosols penetrate or bypassthe mask and fill a medium-sized room within minutes”)
2) by admission on BBC, political lobbying caused WHO to update mask policy (“This point was put to WHO who did not deny it”)
3) despite widespread use of masks in Japan, flu numbers still high
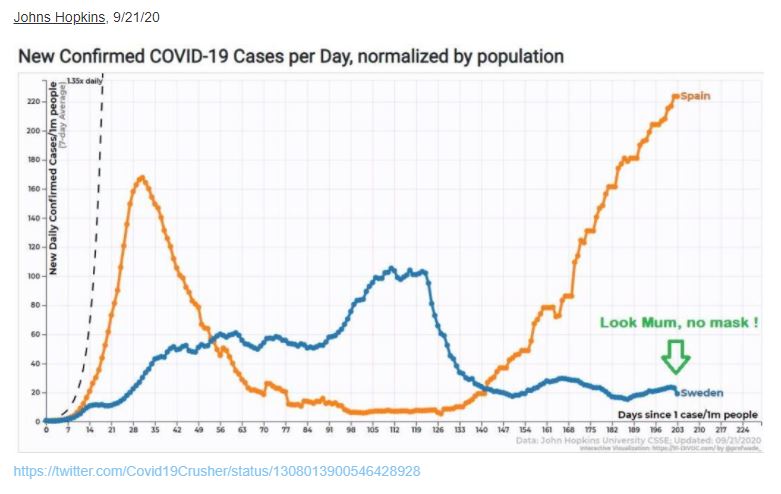
4) many states that mandated face masks (Hawaii, California, Argentina, Spain, France, Japan, Israel…) “saw strong increase in infections…”
5) Austria’s introduction/retraction/re-introduction of face mask mandate saw not influence on rate of infection
6) Kansas department of health attempted to hide fact that counties without mask mandates had lower infection rates than counties that did. Officials tried to manipulate statistics and presentation of data go hide this fact.
7) Hospital studies found surgeons wearing masks during operations didn’t reduce post-op infections
8) Disease and transmission of Covid-19 in children is lower than influenza making face masks “not indicated”
9) Cloth masks used during notorious 1918 flu pandemic “made no difference”
10) Asian countries with low Covid infection/death rates attributed to early border closures, not masks. Same for Scandinavian countries.
— Development of cases after mask mandates references places where infections rose after mandates were introduced, including France and “California, Florida, Hawaii, Argentina, Peru, the Philippines, Spain, Italy, the UK, Israel, Japan, Switzerland and many more.”
RE: Studies claiming efficacy of face masks consists of a list of (6) items and concludes, “Some recent studies argued that cloth face masks are indeed effective against the new coronavirus and could at least prevent the infection of other people. However, most of these studies suffer from poor methodology and sometimes show the opposite of what they claim. Typically, these studies ignore the effect of other measures, the natural development of infection numbers, changes in test activity, or they compare countries with very different conditions.”
RE: Evidence showing risks associated with wearing face masks for prolonged time period include:
1) WHO warns of “side effects” (breathing difficulty, skin rashes…”
2) “face masks significantly reduce the resilience and performance of healthy adults”
3) “severe psychosocial consequences” resulting from mask mandate in Germany
4) “inhalation of chlorine compounds in polyester masks”
5) Recalled masks models that didn’t meet quality standards (“could lead to serious risks”)
6) 13-year-old girl died suddenly in Germany (“autopsy couldn’t exclude CO2 intoxication or a sudden cardiac arrest.”)
7) Children wearing mask during sports classes in China “fainted and died” (autopsies identified “sudden cardiac arrest” as cause of death)
8) Driver in US wearing mask (N95) fainted and crashed his car

VIDEO: MASKS DON'T WORK - Dr. Ted Noel demonstrates how masks don't really work (8/8/2020)
MASKS DON’T WORK is a very effective video demonstration by Dr. Ted Noel, anesthesiologist with 36 years experience wearing masks in operating rooms.
This presentation covers a variety of mask types and underscores the veracity of scientific medical research findings on the subject, statements made by medical, PPE/OSHA safety and expert others (including Dr. Fauci, the CDC and top health officials in Europe, etc.).
Medical Article: Mask Facts - Association of American Physicians & Surgeons (9/26/2020)
Cliff Notes & Pull Quotes:
This article responds to the fact that recommendations made on the issue of universal masking of healthy people have been “published without a single scientific paper or other information provided to support that cloth masks actually provide any respiratory protection.”
This article offers an overview of the with numerous links to a variety of studies and their conclusions re: the following topics:
1) Efficacy – many studies and reviews conclude many problems lead to not recommending masks outside healthcare settings, with some studies warning they “may result in increased risk of infection.” One study showed cloth masks had 97% penetration and medical masks had 44% penetration. In a review of masks and N95 masks against respiratory infection N95s and medical masks were shown to have no statistically significant protective effect against respiratory infection compared to no mask at all.
2) Negative effects – links to studies raising a range of vital concerns with potential for serious negative health consequences resulting from decreased PaO2, increased CO2, moisture retention, self-contamination, mask mouth, other cautions by world authorities, inhalation of chlorine compounds (another study not included here raises concerns re: cotton and sythetic fibers on this issue, along with greater force of inhalation factor) and psychological harm. This section ends by noting:
Unanswered questions
- Can virions escape an evaporating droplet stuck to a mask fiber?
- What are long-term health effects on HCW, such as headaches, arising from impeded breathing?
- Are there negative social consequences to a masked society?
- Are there negative psychological consequences to wearing a mask, as a fear-based behavioral modification?
- What are the environmental consequences of mask manufacturing and disposal?
[Note: for additional facts related to these concerns, see toggles titled, “EMPLOYER MUST WATCH — VIDEO: The Science of Masks” and “EMPLOYER MUST READ — EDITORIAL: Human factors expert: masks may increase business liability (6/30/2020)]
3) Positive mask studies – provides links to studies with brief summaries, as well as many notes regarding problems in relation to the research and/or its findings. This section ends by noting:
- Many studies ignore the effect of other measures, the natural development of infection numbers, changes in test activity, or they compare countries with very different conditions.
4) Conclusions from organizations – includes conflicting statements by world authorities that serve as guidelines and the very different approaches around the world to this issue.
5) Final thoughts – makes points about general concerns and ideas. [note, while previous sections referenced important findings about vitamin D, immune function and other related facts, this section does not address this and other essential material raised in greater detail under toggle titled, “EMPLOYER MUST WATCH — VIDEO: The Science of Masks”]
6) Footnote – handwashing and facts in relation to surface transmission
REVIEW: Masks are neither effective nor safe: A summary of the science (7/6/2020)
Cliff Notes & Pull Quotes:
This is a review of peer-reviewed medical literature that focuses on effectiveness of facemasks (and related safety data) with an eye on risk-benefit analysis related to potential impacts on immunological and physiological health. More than 40 studies are cited.
SUMMARY: “The use of face masks, whether cloth, surgical or N95, creates a poor obstacle to aerosolized pathogens…masks impede the necessary volume of air intake required for adequate oxygen exchange, which results in observed physiological effects that may be undesirable…Even 6- minute walks…resulted in dyspnea…masks serve more as instruments of obstruction of normal breathing, rather than as effective barriers to pathogens. Therefore, masks should not be used by the general public, either by adults or children, and their limitations as prophylaxis against pathogens should also be considered in medical settings.”
Topics covered in this feature include:
Are masks effective at preventing spread of respiratory pathogens? Some findings included: (1) “Compared to no masks, there was no reduction of influenza-like illness cases or influenza for masks in the general population, nor in healthcare workers.” and (2) “…both N95 respirators and surgical masks “resulted in no significant difference in the incidence of laboratory confirmed influenza.” and (3) “…both randomized controlled trials and observational studies of N95 respirators and surgical masks used by healthcare workers did not show benefit against transmission of acute respiratory infections. It was also found that acute respiratory infection transmission “may have occurred via contamination of provided respiratory protective equipment during storage and reuse of masks and respirators throughout the workday.”
What about Airflow? Some findings included: (1) “…there have been farther transmission of virus-laden fluid particles from masked individuals than from unmasked individuals, by means of “several leakage jets, including intense backward and downwards jets that may present major hazards,” and a “potentially dangerous leakage jet of up to several meters.” and (2) “…both surgical masks and cloth masks had farther brow jets (unfiltered upward airflow past eyebrows) than not wearing any mask at all…” and (3) “…both N95 and surgical masks, it was found that expelled particles from 0.03 to 1 micron were deflected around the edges of each mask, and that there was measurable penetration of particles through the filter of each mask.”
What about Penetration through masks? Some findings include: (1) ““…Medical masks, general masks, and handkerchiefs were found to provide little protection against respiratory aerosols.” and (2) “…penetration of cloth masks by particles was almost 97% and medical masks 44%”
RE: N95 Respirators? Some findings include: (1) “These are made with a 0.3 micron filter. (12) N95 respirators are so named, because 95% of particles having a diameter of 0.3 microns are filtered by the mask forward of the wearer, by use of an electrostatic mechanism. Coronaviruses are approximately 0.125 microns in diameter.” and (2) “…N95 respirators did not provide superior protection to facemasks against viral infections or influenza-like infections.” and (3) “Pregnant healthcare workers were found to have a loss in volume of oxygen consumption by 13.8%…17.7% less carbon dioxide was exhaled.” and (4) “Healthcare workers’ N95 respirators were measured by personal bioaerosol samplers to harbor influenza virus.”
RE: Surgical Masks? Some findings included: (1) “…surgical masks offered no protection at all against influenza.” and (2) “Use of masks in surgery were found to slightly increase incidence of infection over not masking…” and (3) “…medical masks have a wide range of filtration efficiency, with most showing a 30% to 50% efficiency.” and (4) “…neither surgical nor cotton masks effectively filtered SARS-CoV-2 during coughs by infected patients.” And more viral particles were found on the outside than on the inside of masks tested.” and (5) “…respiratory pathogens were found on the outer surface of used medical masks, which could result in self-contamination. The risk was found to be higher with longer duration of mask use.”
RE: Cloth Masks: Some findings included: (1) “…have low efficiency for blocking particles of 0.3 microns and smaller. Aerosol penetration through the various cloth masks examined in this study were between 74 and 90%. Likewise, the filtration efficiency of fabric materials was 3% to 33%” and (2) “Healthcare workers wearing cloth masks were found to have 13 times the risk of influenza-like illness than those wearing medical masks.” and (3) “Healthcare workers wearing cloth masks had significantly higher rates of influenza-like illness after four weeks of continuous on-the-job use, when compared to controls.” and (4) “…increased rate of infection in mask-wearers may be due to a weakening of immune function…Surgeons have been found to have lower oxygen saturation after surgeries even as short as 30 minutes…Low oxygen induces hypoxia-inducible factor 1 alpha (HIF-1)… in turn down-regulates CD4+ T-cells. CD4+ T-cells, in turn, are necessary for viral immunity.”
RE: protection against Covid-19: New England Journal of Medicine states: “…“We know that wearing a mask outside health care facilities offers little, if any, protection from infection…The chance of catching Covid-19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.”
RE: masks during exercise: Some findings include: (1) Surgical mask wearers had significantly increased dyspnea after a 6-minute walk than non-mask wearers.” and (2) “Researchers are concerned about possible burden of facemasks during physical activity on pulmonary, circulatory and immune systems…”
EMPLOYER "MUST READ" -- STUDY: Masks, false safety and real dangers, Part 1: Friable mask particulate and lung vulnerability (09/2020 - preprint/early release)
Cliff Notes & Pull Quotes:
This “Part One” study raises serious health concerns about universal masking in what it accurately defines as a “society-wide experiment.”
ABSTRACT: “There is no biological history of mass masking until the current era. It is important to consider possible outcomes of this society-wide experiment. The consequences to the health of individuals is as yet unknown. Masked individuals have measurably higher inspiratory flow than non-masked individuals. This study is of new masks removed from manufacturer packaging, as well as a laundered cloth mask, examined microscopically. Loose particulate was seen on each type of mask. Also, tight and loose fibers were seen on each type of mask. If every foreign particle and every fiber in every facemask is always secure and not detachable by airflow, then there should be no risk of inhalation of such particles and fibers. However, if even a small portion of mask fibers is detachable by inspiratory airflow, or if there is debris in mask manufacture or packaging or handling, then there is the possibility of not only entry of foreign material to the airways, but also entry to deep lung tissue, and potential pathological consequences of foreign bodies in the lungs.”
Historical context provided:
1) Nose and mouth are “gateways” to lungs for all land vertebrates. No history exists of voluntary/involuntary obstructing/partially obstructing airways and lungs of a species so it is unknown how entire species might adapt/survive the novel practice.
2) In some countries, human self-masking has become common (by government insistence, regulation by employers/educational system and/or social pressure).
3) Out of “abundant fear” and desire for protection from Covid-19, people are being coerced and/or pressured to wear “face coverings” to purportedly “slow the spread of Covid-19.”
4) General public is using disposable surgical masks and variety of cloth masks / other coverings, all of which have not been historically worn outside hospital settings in western hemisphere.
5) “Prior research has overwhelmingly shown that there is no significant evidence of benefits of masks, particularly regarding transmission of viral infections, and…well-established risks.”
Scientific context provided:
1) OSHA has determined optimal oxygen intake absent any obstruction of airways is between 19.5-23.5% and anything less than 19.5% is to be labeled “not safe for workers.”
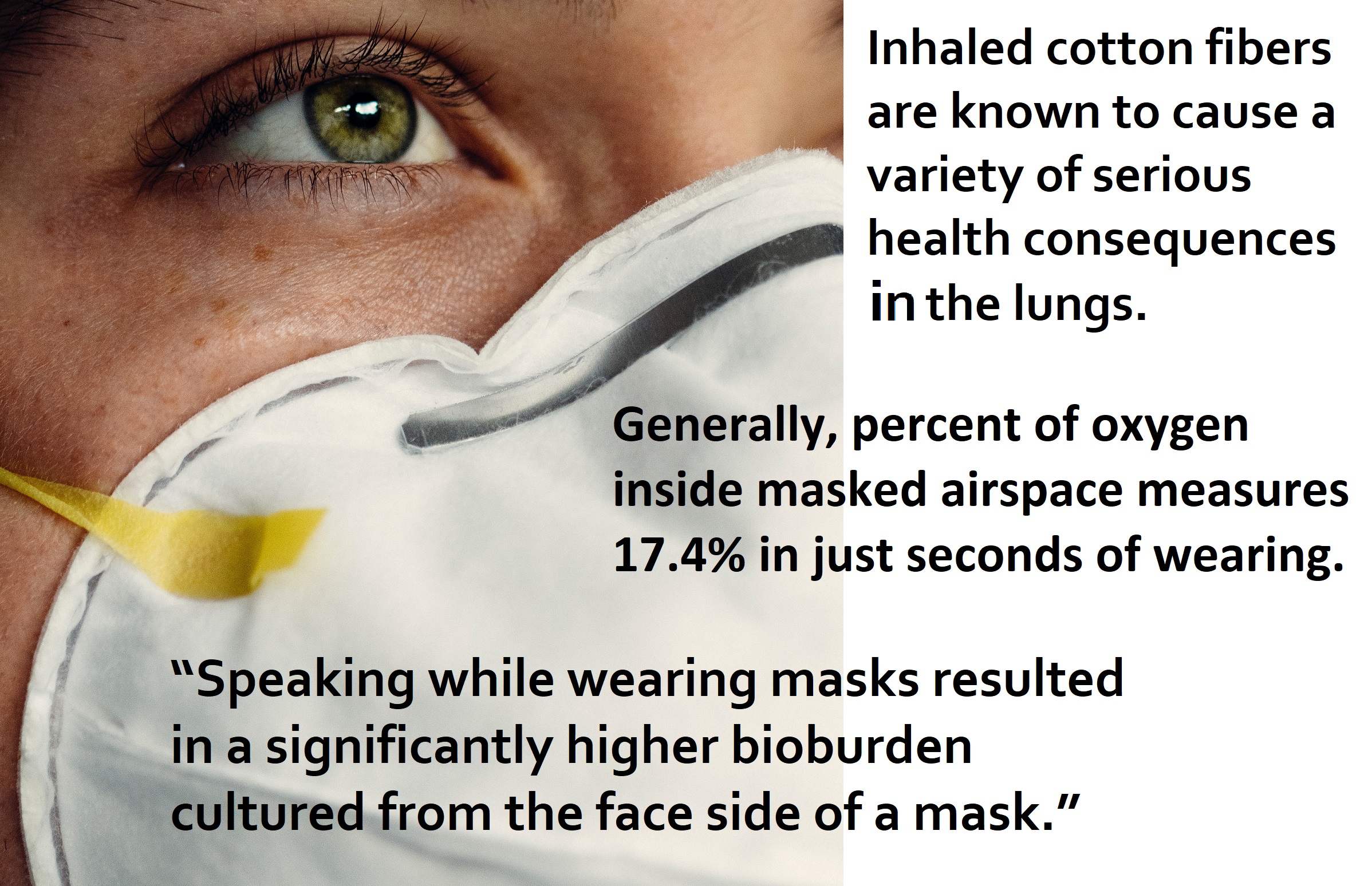
2) Generally, percent of oxygen inside masked airspace measures 17.4% in just seconds of wearing.
3) Observation shows “maximal voluntary ventilation and maximal inspiratory pressure increase during lower availability of oxygen at ascent in altitude (and those living at altitude).
4) Humans have developed ability to sense changes in oxygen concentration and adapt; to ensure needs of body (“lower ambient oxygen and increased carbon dioxide stimulates ventilation”).
5) “As a compensatory mechanism, inspiratory flow is measurably higher in mask-wearers than in controls.“
Questions raised:
1) “If inspiratory flow is increased over normal while wearing a mask, is every fiber attached to one’s facemask secure enough not to be inhaled into the lungs of the mask-wearer?”
2) “Is it good enough for a majority of these fibers to be secure? Or must every part of every mask fiber of every mask be secure at all times?”
Materials used in masks, prefaced by known hazards:
1) Inhaled cotton fibers are known to cause a variety of serious health consequences in the lungs.
2) Textile workers are discussed in association with cotton and silk fibers, COPD, asthma and Byssinosis (pulmonary syndrome) and authors note “unmasked textile workers would not have such high inspiratory flow as masked individuals).
3) The above makes clear the need for “fibers, debris and other particulate attached to cloth masks…stay entirely intact; every fiber…part of every fiber…throughout every breath, at all times, even down to the size of nanometers.”
4) Disposable surgical masks contain “synthetic fibers, including polymers such as polypropylene, polyurethane, polyacrylonitrile, polystyrene, polycarbonate, polyethylene or polyester.”
5) Research has shown “a correlation between inhalation of synthetic fibers and various bronchopulmonary diseases.” (lists asthma, chronic bronchitis, chronic pneumonia and more)
6) Those exposed to synthetic fibers in ambient air were shown to have developed lung illnesses (some that could be reversed but others “had already proceeded to pulmonary fibrosis).
7) “Bioburden of masks has also been established,” including that “Speaking while wearing masks resulted in a significantly higher bioburden cultured from the face side of a mask.”
Possible Risk of Pulmonary Fibrosis:
1) It is among the “worst diseases that can be suffered or witnessed. It kills exceedingly slowly…suffocates the victim very gradually,” and that there is no treatment or cure available
2) “The 5-year survival rate is only 20%. The only remedy against this scourge is diligent prevention of small and microscopic inhaled foreign bodies.”
3) “Inhaled particles, particularly nanoparticles, can begin the process of pulmonary fibrosis by forming free radicals such as superoxide anions. The resulting oxidative stress promotes inflammatory response…”
4) “Particles of nanometer to micrometer size have been implicated as causative agents in pulmonary fibrosis. Airborne inhaled nano-size particles are especially dangerous for the lungs…[are small enough to] enter blood and lymph, reaching the cardiovascular system, spleen, bone marrow …” and more.
Methods and key findings:
1) Macro- and Microscopic examination of “concave face side of a variety of new masks, taken directly out of their packaging from the manufacturer, not yet worn. However, the cloth mask below was worn for one day, and then laundered, and never worn again.”
2) Masks examined included a) Cup b) Surgical c) two different types of N95 d) one Cloth (worn one day, laundered and not used again)
3) Images shown of each mask examined were taken at 40x to 100 x magnification and reveal particulates and soiled appearing fibers; cloth mask showed particulate and loosened fibers.
4) Re: additional photo of lightly used hospital mask “illuminated by a consumer LED flashlight” authors note, “…when masks are used, particulate and fibers may become further loosened.”
5) “All of the masks showed partially loose fibers in nearly every visual field.”
6) “The first N-95 [with valve] showed the fewest loose particles” and “…cloth mask had more loose fibers than the others, typically 4 or 5 partially loose or dangling fibers that were compressible toward the weave in each visual field.”
Conclusion points made:
1) Trained surgical staff never touch any part of mask (save loops/nose bridge) because, if they do, “mask is considered useless and is to be replaced.
2) General public touches masks [rendering them useless/to be replaced].
3) Masks just removed from packaging are shown by this study “to contain particulate and fiber that would not be optimal to inhale.”
4) Inhalation risks like those associated with body’s attempt to get needed oxygen [breathing] with “mostly and closely covered orifices” are concerning for those with interest in protecting “pulmonary health, without inhalation of unwanted particulate.”
5) People breathe more deeply and forcefully when airway is partially obstructed [by masking]; this phenomenon combined with particles found in this study can raise “risk of a dangerous level of foreign material entering lung tissue.”
6) These particles can either become loose “to lodge in the lungs of the wearer” or “accumulate during use, to the burden (both biological and debris) of non-mask material carried on the inside of the mask.”
7) This study suggests more research should be done re: “macrophage response and other immune and inflammatory and fibroblast response to such inhaled particles” from masks.
8) This study cautions, “If widespread masking continues, then the potential for inhaling mask fibers and environmental and biological debris continues on a daily basis for hundreds of millions of people. This should be alarming for physicians and epidemiologists knowledgeable in occupational hazards.”
EMPLOYER "MUST READ": PPE & OSHA Environmental Safety expert's video destroys mask narrative, raises liability & health concerns (7/3/2020)
Tammy K. Herrema Clark DESTROYING the mask narrative especially masks and children!
Cliff Notes & Transcribed Quotes:
WHITE PAPER Still No Conclusive Evidence Justifying Mandatory Masks (8/12/2020)
Cliff Notes & Pull Quotes:
This is a follow-up to the white paper, “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy.” (which closed with, “We pledge to publish all letters, guest commentaries, or studies refuting [Rancourt’s] general premise that this mask-wearing culture and shaming could be more harmful than helpful.” and which is also presented on this page – see toggle below this one).
This new feature follows through on the closing promise to previous article and makes the following statement, “We received many submissions against and for Rancourt’s paper. After reviewing the attempted refutations, we remain resolute in our original support for his conclusions. Not one proved Rancourt’s analysis of the randomized controlled tests to be false or misleading. Nor did any of the attempted refutations answer or overcome any of Rancourt’s concerns regarding potential harm from mandated mask wearing.”
“However, in the spirit of open debate and sharing opposing views, we provide links to several of the submitted refutation efforts below. While some submitters resorted to unpersuasive ad hominem attacks on Rancourt, we stand by Rancourt’s scientific and academic credentials, training, experience, and capabilities to provide the analysis and review of said RCT’s.”
The feature then presents a variety of contentions and related commentary, in direct response, adding, “Not one of the seven publications on RCT’s Rancourt reviewed, or all of them combined, warrants implementing (let alone attempting to enforce) mask mandating as a mitigation policy for COVID-19. Rancourt takes a dispassionate view of the evidence being reported within the RCT literature. He does not rely on terms such as “seem to,” “indicates,” “pretty likely,” “much less likely,” “may,” or “some evidence to support.” Rather, Rancourt selected the science-based disclaimers within each of the RCT analyses to prove his point that there is no policy-grade evidence that masks work.”
It also calls attention to OSHA (as does this video by PPE and OSHA Environmental expert we have posted on this page, along with a transcript to save time – it’s 49 minutes long), as follows:
“OSHA has remained curiously silent relative to COVID-19 and mask-wearing safety in the workplace, nor has it explained suddenly waiving its safety standards otherwise strictly imposed on employers who require mask/respirator-wearing by employees in the workplace. Mandatory government oversight of this workplace practice confirms there are substantive dangers associated with mask-wearing for prolonged periods, requiring rigorous protocols to mitigate potential health hazards.
(1) OSHA strictly regulates the airflow, temperature and humidity, amount of oxygen that must be available throughout the work environment, behind the respirator itself, and in the bloodstream, while wearing respirators. This is especially true in surgery rooms, where the environment is very specifically regulated for optimum oxygen availability, intake, CO2 expulsion, etc.
(2) A complete medical evaluation must be completed on each employee required to wear a respirator during work hours to ensure his/her ability to safely wear the device for prolonged periods.
(3) Employers must provide a “Respirator Program” for their facilities that meet OSHA requirements for employee safety on penalty of stiff fines, even shutdowns.
Knowing the differences in approximate sizes of viruses, particles, aerosols, droplets, and mask pores is useful to assess the risks inherent in cloth masks. Viruses are measured in nanometers or microns (1 nanometer is 1/billionth of a meter, while 1 micron is 1/millionth of a meter) and viruses typically measure 125 nanometers or .125 micron. Viruses are carried as part of larger particles that range in measurement between 0.02 – 0.14 microns. Particles are transported in aerosols and droplets. Aerosols are typically less than 5 microns, while droplets are often larger, ranging between 5 – 10 microns.
Mask pores have a wider range of diameter sizes, anywhere from 80-500 microns. While viruses always travel as part of larger particles carried in aerosols or droplets, mask pores’ larger circumference arguably can’t prevent most flow through of smaller aerosol particles that carry ever smaller bacteria and viruses.
Supporting documentation for this compilation is available at the end of this August editorial titled “Disturbingly COVID Incurious,” by Kathleen McCarthy.”
It then concludes, “In his follow-up paper titled “Face masks, lies, damn lies, and public health officials: ‘A growing body of evidence,’” Rancourt is doubling down on his resolve that mandating mask-wearing for the public is not only unsupported by science, it is irresponsible policy by authorities. He writes, “I prove that there is no policy-grade evidence to support forced masking on the general population, and that all the latest-decade’s policy-grade evidence points to the opposite: NOT recommending forced masking of the general population. Therefore, the politicians and health authorities are acting without legitimacy and recklessly.” Rancourt’s follow-up paper includes his extensive credentials.”
MEDICAL ARTICLE: The Risk to Benefit Ratio of Wearing Masks (6/30/2020)
Read medical article — Jim Meehan, M.D.
Cliff Notes & Pull Quotes:
Summary: Dr. Meehan performs an analysis showing high risk to low benefit of healthy people wearing face masks.
Premise of article: “All medical interventions should be weighed according to a full accounting and analysis of the risks and benefits of the intervention. Unfortunately, rather than providing the public with a full and fair assessment of the pros-and-cons and risks-and-benefits, the CDC, WHO, and many public health “experts” have lied (Fauci in March), confused, and frequently changed their positions and rationales for recommending community wearing of medical masks. Furthermore, the experts have been willfully negligent in fully informing the public of the risks of wearing medical masks.”
Benefits listed: “On the benefits side of the ratio, we have some evidence that suggests surgical and cloth masks provide some benefits in blocking respiratory droplets and the viral particles they contain. The scientific research literature demonstrates that N95 masks block 95% of respiratory droplets, surgical masks 44%, and cloth masks 3%. The first point that should be clear is that more viral particles pass through the mask than are blocked, and cloth masks are fairly worthless. In fact, cloth masks are so ineffective and more likely to mislead the wearer into not guarding coughs and sneezes, that they are probably worse than going mask-less while practicing appropriate guarding behaviors. Regardless of their limited ability to block respiratory droplets and viral particles, masks add almost nothing to the prevention of viral transmission achieved by frequent hand washing and social distancing practices. Therefore, the overall benefit of masks contributes almost nothing to the picture, and the benefit side of the ratio is very small.”
Risks listed: “On the risk side, medical masks significantly increase the risk of:
- Lowering arterial oxygen (which causes a long list of adverse effects, including increasing the infectivity and severity of a SARS CoV-2 infection)
- Increasing arterial carbon dioxide (which causes an equally long list of adverse effects)
- Masks must be worn, fit, handled, and carefully maintained as sterile, otherwise they become a mechanism for self-inoculation and spreading of far more diseases than CoVID-19.
- Anyone that fails to wash their hands thoroughly both before and after touching their mask is increasing infection and transmission.
- Masks are warm, moist traps for viruses and a breeding ground for bacteria and fungi, any one of which could cause life-threatening respiratory diseases and pneumonia.
- Medical masks are SINGLE use medical devices. When they are reused, which is exactly what is happening in the public, they increase infections and transmission.
- Re-breathing viral particles increases viral load and increases the severity of viral disease.
I could continue, but I think that list is enough to establish the fact that the “risk number” is sufficiently large.”
Conclusion: “You don’t have to have an advanced degree in math or the sciences to understand that the risk to benefit ratio does not support community wearing of medical masks.”
Recommendation: “If you are vulnerable and worried, wash your hands frequently and stay six feet away from anyone you don’t know or trust to be uninfected. The rest of us will do the only thing that has ever worked against pandemic diseases. We will bravely encounter the virus, allow our healthy immune systems to eradicate the virus, develop lifelong immunity, and allow ourselves to become contributors to herd immunity. We will protect those who cannot protect themselves.”
EDITORIAL: Dr. Russel Blaylock: Face Masks Pose Serious Risks To The Healthy – Hypoxia And Hypercapnia (5/13/2020)
Cliff Notes & Pull Quotes:
WHITE PAPER: Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy (7/11/2020)
Read article by Dennis P. Rancourt, Ph.D.
Cliff Notes & Pull Quotes:
This article does a great job of citing extensive randomized controlled trial (RCT) studies and meta-analysis reviews of RCTs which show masks and respirators to be ineffective at preventing “respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles.”
Also reviewed are known physics and biology that point to masks being ineffective in light of what is known about viral respiratory diseases: “The main transmission path is long-residence-time aerosol particles (< 2.5 μm), which are too fine to be blocked, and the minimum-infective dose is smaller than one aerosol particle.”
CONCLUSION: The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.”
NEWS: Masks may actually increase your coronavirus risk if worn improperly, surgeon general warns (3/2/2020)
Cliff Notes & Pull Quotes:
CNN reports on Surgeon General Dr. Jerome Adams’ statements regarding face masks, including:
1) warning people might increase risk of infections if not wearing facemasks properly.
2) Stating,”You can increase your risk of getting it by wearing a mask if you are not a health care provider.”
3) Noting that people, “…tend to touch their faces a lot and actually can increase the spread of coronavirus.”
4) Advising people stop buying masks while recommending they wash hands often, avoid touching eyes/nose/mouth with unwashed hands and disinfect surfaces.
MEDICAL ARTICLE: Why Face Masks Don't Work (10/18/16)
Cliff Notes & Pull Quotes:
This article about the efficacy of wearing face masks is very technical but also very readable and scientifically based. Specifically, it addresses their use in the dental profession.
SUMMARY: “The primary reason for mandating the wearing of face masks is to protect dental personnel from airborne pathogens. This review has established that face masks are incapable of providing such a level of protection. Unless the Centers for Disease Control and Prevention, national and provincial dental associations and regulatory agencies publically admit this fact, they will be guilty of perpetuating a myth which will be a disservice to the dental profession and its patients. It would be beneficial if, as a consequence of the review, all present infection control recommendations were subjected to the same rigorous testing as any new clinical intervention. Professional associations and governing bodies must ensure the clinical efficacy of quality improvement procedures prior to them being mandated. It is heartening to know that such a trend is gaining a momentum which might reveal the inadequacies of other long held dental infection control assumptions. Surely, the hallmark of a mature profession is one which permits new evidence to trump established beliefs. In 1910, Dr. C. Chapin, a public health pioneer, summarized this idea by stating, “We should not be ashamed to change our methods; rather, we should be ashamed not to do so.” 36 Until this occurs, as this review has revealed, dentists have nothing to fear by unmasking. OH”
DETAILS:
The article opens by exploring historical basis for wearing face masks and contrasting this with modern studies and science concluding, “The above illustrate the developing concerns that many infection control measures have been adopted with minimal supporting evidence. To address this fault, the authors of a 2007 New England Journal of Medicine (NEJM) article eloquently argue that all safety and quality improvement recommendations must be subjected to the same rigorous testing as would any new clinical intervention. 10 Dr. R. MacIntyre, a proponent of this trend in infection control, has used her research findings to boldly state that, “it would not seem justifiable to ask healthcare workers to wear surgical masks.” 4 To understand this conclusion it is necessary to appreciate the current concepts relating to airborne transmissions.”
Next, it discusses droplet v. aerosol transmission and concludes, “raditionally face masks have been recommended to protect the mouth and nose from the “droplet” route of infection, presumably because they will prevent the inhalation of relatively large particles. 11 Their efficacy must be re-examined in light of the fact that aerosols contain particles many times smaller than 5 microns. Prior to this examination, it is pertinent to review the defence mechanism of the respiratory tract.”
It discusses respiratory defenses stating, “…readers are reminded that; coughing, sneezing, nasal hairs, respiratory tract cilia, mucous producing lining cells and the phagocytic activity of alveolar macrophages provide protection against inhaled foreign bodies including fungi, bacteria and viruses. 13 Indeed, the pathogen laden aerosols produced by everyday talking and eating would have the potential to cause significant disease if it were not for these effective respiratory tract defences.” It concludes, “The respiratory tract has efficient defence mechanisms. Unless face masks have the ability to either enhance or lessen the need for such natural defences, their use as protection against airborne pathogens must be questioned.”
It discusses use historical use and functionality, concluding, “Literature reviews have confirmed that wearing a mask during surgery has no impact whatsoever on wound infection rates during clean surgery. 22,23,24,25,26 A recent 2014 report states categorically that no clinical trials have ever shown that wearing a mask prevents contamination of surgical sites. 26 With their original purpose being highly questionable it should be no surprise that the ability of face masks to act as respiratory protective devices is now the subject of intense scrutiny. 27 Appreciating the reasons for this, requires an understanding of the structure, fit and filtering capacity of face masks.”
Re: structure and fit, it states, “No matter how well a mask conforms to the shape of a person’s face, it is not designed to create an air tight seal around the face. Masks will always fit fairly loosely with considerable gaps along the cheeks, around the bridge of the nose and along the bottom edge of the mask below the chin. 21 These gaps do not provide adequate protection as they permit the passage of air and aerosols when the wearer inhales. 11,17 It is important to appreciate that if masks contained filters capable of trapping viruses, the peripheral gaps around the masks would continue to permit the inhalation of unfiltered air and aerosols. 11″
Re: filtering, it cites different studies with technical results of masks and states, “It should be concluded from these and similar studies that the filter material of face masks does not retain or filter out viruses or other submicron particles. 11,31 When this understanding is combined with the poor fit of masks, it is readily appreciated that neither the filter performance nor the facial fit characteristics of face masks qualify them as being devices which protect against respiratory infections. 27 Despite this determination the performance of masks against certain criteria has been used to justify their effectiveness.2 Accordingly, it is appropriate to review the limitations of these performance standards.”
Re: performance standards, it states, “Face masks are not subject to any regulations.” It details a great many technical aspects related to unregulated aspects of masks, testing, etc. and states, “Although these tests are conducted under the auspices of the American Society of Testing and Materials (ASTM) and often produce filtration efficiencies in the range of 95-98 %, they are not a measure of a masks ability to protect against respiratory pathogens. Failure to appreciate the limitations of these tests combined with a reliance on the high filtration efficiencies reported by the manufacturers has, according to Healthcare in BC, “created an environment in which health care workers think they are more protected than they actually are.” 21 For dental personnel the protection sought is mainly from treatment induced aerosols.”
Re: dental aerosols, it states, “For approximately 40 years it has been known that dental restorative and especially ultrasonic scaling procedures produce aerosols containing not only blood and saliva but potentially pathogenic organisms. ” It concludes, “The most effective measures for reducing disease transmission from dental aerosols are pre-procedural rinses with mouthwashes such as chlorhexidine, large diameter high volume evacuators, and rubber dam whenever possible. 33 Face masks are not useful for this purpose, and Dr. Harrel believes that dental personnel have placed too great a reliance on their efficacy. 34 Perhaps this has occurred because dental regulatory agencies have failed to appreciate the increasing evidence on face mask inadequacies.”
Re: inadequacies of masks, it cites more than a dozen studies demonstrating face masks cannot prevent wearer from inhaling aerosols. It states, “Health care workers have long relied heavily on surgical masks to provide protection against influenza and other infections. Yet there are no convincing scientific data that support the effectiveness of masks for respiratory protection. The masks we use are not designed for such purposes, and when tested, they have proved to vary widely in filtration capability, allowing penetration of aerosol particles ranging from four to 90%.” 35″ It concludes, “A significant inadequacy of face masks is that they were mandated as an intervention based on an assumption rather than on appropriate testing.
Note, after reading this feature, you may want to see a related feature that includes the following content:
“The concept of masks has been studied for a long time, especially in the dental community. They obviously work very closely with people, and a lot of literature has been written. There are some studies out there that show that dentists who wear masks and face shields have the same antibodies to the plethora of influenza and respiratory syncytial viruses, which sort of show that the masks were not effective in preventing the disease transmission in these types of professionals,” Barbour said.
Some evidence indicates an increased risk of influenza-like illness transmission associated with cloth masks, stated Barbour.
“We have one randomized controlled study on cloth masks, and the results of that study were that the people wearing the cloth masks were actually more likely to contract the influenza-like illnesses. My attitude towards masks is there’s no real compelling evidence that they do work, and I think that that was sort of relatively accepted before 2020 now suddenly masks are being mandated,” Barbour said.”
WHITE PAPER: The surgical mask is a bad fit for risk reduction (5/17/16)
Read White Paper — National Center for Biotechnology Information, U.S. National Library of Medicine (NCBI)
Cliff Notes & Pull Quotes:
Part of the premise of this paper is communicated as follows: “The surgical mask communicates risk. For most, risk is perceived as the potential loss of something of value, but there is another side to risk, memorably formulated by Beck in his Risk Society.2 Beck states that risk society is “a systematic way of dealing with hazards and insecurities induced and introduced by modernisation itself.”2 For Beck, risk occurs not only in the form of threat and possible loss, but also in society’s organized management and response to these risks, which create a forwarding of present risk into the future. Furthermore, Beck writes of the “symptoms and symbols of risks” that combine in populations to create a “cosmetics of risk.” He suggests that people living in the present moment conceive of risk in terms of the physical tools used to mitigate risk while still “maintaining the source of the filth.” Beck critiques the cosmetics of risk as measures that are not preventive but rather act as a “symbolic industry and policy of eliminating the increase in risks.” I propose that the surgical mask is a symbol that protects from the perception of risk by offering nonprotection to the public while causing behaviours that project risk into the future.” [emphasis added]
History of surgical masks is presented in relation to the psychology of fear and public policy: “Western society has already emerged into a present reality in which citizens are conditioned to want masks on the basis of media representations of pandemics. The same annex on public health measures refers to the “false sense of security” that a mask can psychologically provide,9 but the converse is the real risk posed to a government unable to mollify its population.”
Feature concludes: “We act out our collective anxiety about pandemics by wearing masks even when there isn’t a pandemic,1 but wearing masks reinforces the idea of a possible future of pandemic. The problem of affect in political terms is a contagious one: fear spreads among the public, leading to intensification of risk management — the classic example being 9/11 and the war on terrorism. Fear of infective risk spreading communicably becomes an ironic pun. Pandemics occurred in 1918, 1957, 1968, 2003 and 2009. Thus, the conversation changes from if the next pandemic will occur to when the next pandemic will occur. Because we are currently “between pandemics,” our existence is book-ended by the realized threats of the past and the reasonable threats of the future — to our detriment, with this detriment masked by the surgical mask itself.”

MEDICAL REVIEW: Face masks to prevent transmission of influenza virus: A systematic review,” Epidemiology and Infection (2010)
Read Medical Review — Cowling, B. et al. (2010) “Face masks to prevent transmission of influenza virus: A systematic review,” Epidemiology and Infection, 138(4), 449-456.
Cliff Notes & Pull Quotes:
This medical review is directly referenced as part of the white paper, “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” as follows: “None of the studies reviewed showed a benefit from wearing a mask, in either HCW or community members in households (H). See summary Tables 1 and 2 therein.”
RE: all studies/medical reviews cited and discussed in “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” the following general conclusion is drawn (in addition to otherwise going into many aspects worth reading):
“Conclusion Regarding That Masks Do Not Work
No RCT study with verified outcome shows a benefit for HCW or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions.
Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
Masks and respirators do not work.”
VIDEO: Dr. Jen Ashton Breaks Down Face Masks (5/15/2020)
Transcription:
“We put surgical masks on sick people to protect healthy people around them. They serve an emotional or psychological benefit for people because people feel more protected. The reality is they don’t really provide us with protection. “
This health expert breaks down confusion about face masks: amid the ongoing coronavirus outbreak.
“So, there are basically two types of masks: there’s surgical masks and there are masks called N95 respirators. Let’s start with the surgical masks. In a hospital setting – I’m a surgeon – I do real surgery, when I go into the operating room and I put a surgical mask on, it is not to protect myself from getting sick in a sterile environment. It is to protect the patient that I’m operating on, in case I spit while I’m talking, or cough, or sneeze. Surgical masks that you see all over television and video – they do not block out the tiny particle size of coronaviruses or influenza virus. They don’t. Those viruses can pretty much go right through those masks.
Now, you would ask, well, then, why, if you’re sick would – do those masks do anything? Simply as a barrier. It could be a plastic wall. It could be, you know, a scarf. But masks are just convenient to give to a patient if they’re coughing or sneezing.
Then you go to the N95 respirator. There are a bunch of different models. They come in different sizes, different shapes. Those are for healthcare providers when they are taking care of a sick person with a high impact respiratory pathogen. They’re called N95s because they block out 95% of viral particles. You have to be fit tested for those masks, a specialized process. If you’re not, they can actually also do more harm than good. They also have to be worn a certain way. They’re single-use only. So, when they start to get wet, which generally happens in about a half an hour, people need to change them. So those are for healthcare providers when they are taking care of a patient with known or suspected infectious respiratory disease. I totally get that people feel more comfortable if they have a mask on, but the science just doesn’t support that.”
While the CDC maintains the general public does not need to wear masks, U.S. health officials have said 300 million N95 masks are needed for healthcare workers who will be treating possibly infected patients.
“It’s talking about a distinction between concern for me as an individual – me, myself and I – and my role to protect those around me. So it’s a difference of being selfish and selfless. Or thinking of the needs of others before the needs of oneself. However you want to describe it, that’s pretty much what the surgical mask issue comes down to.”
VIDEO: Post-COVID Analysis: Pandemic Over / Casedemic Continues (9/4/2020)
Cliff Notes & Pull Quotes:
Dr. Ben Edwards presents a post-COVID Analysis using stricly data, research and material facts that demonstrate the pandemic is now over while a “case-demic” continues. The entire video contains valuable information however, as relates to masks, below is a transcript of the portion of the video limited to this topic:
– 14:40 “…so if you’re asymptomatic, you don’t spread the infection. Here’s New England Journal of Medicine, May of 2020: ‘We know that wearing a mask outside of healthcare facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to Covid-19 as face-to-face contact within six feet of a patient and sustained for at least a few minutes and some say more than ten minutes.’ Let me repeat that – face-to-face contact, within six feet for many minutes; not walking by someone in the grocery store, down the sidewalk or anywhere else. And they have to be symptomatic; and you have to be sitting there having lots of conversation[again reading from article], ‘The chance of catching Covid-19 from passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.”
– 13:30 “From the same article, ‘It’s also clear that masks serve symbolic roles. They help increase healthcare workers perceived sense of safety and wellbeing. Although such reactions may not be strictly logical, we are all subject to fear and anxiety, especially during times of crisis. One might argue that fear and anxiety are better countered with data and education, than with a marginally beneficial mask.’”
– 12:50 “We already talked about 17 studies from Dr. Blaylock that he looked at and reviewed the mask – no benefit. And 50 studies that Dr. Tenpenny, um, she’s published this – go review those 50 studies that she found. There’s Dr. Paul Rancourt. All the studies he found all say the same thing. This is a doctor in London, Jenny Harries, deputy chief medical officer – ‘actually, masks can trap the virus and make it even worse.’ Common sense will tell you, your exhaust is building up on the mask – it’s dirty; it’s condensation; there’s – viral particles could build – according to her opinion, that could increase your risk of infection and then, beyond her opinion, here’s a published article that says the same thing, ‘infection outcomes were highest in the cloth mask arm…’ This study is a randomized controlled trial of cloth masks and the results caution against use of cloth masks because ‘moisture retention and reuse of cloth masks and poor filtration may result in increased risk of infection.’ British Medical Journal [BMJ]…that is from 2015.”
MEDICAL ARTICLE: Face masks for the public during the covid-19 crisis (4/9/2020)
Cliff Notes & Pull Quotes:
This epidemiologist raises serious questions re: healthy people being mandated to wear face masks.
Article opens with: “…the precautionary principle aims at preventing researchers and policy makers from neglecting potentially-harmful side effects of interventions. Before implementing clinical and public health interventions, one must actively hypothesise and describe potential side effects and only then decide whether they are worth being quantified on not.”
He then recognizes two potential side effects that have already been acknowledged include a false sense of security that may lead to reduced compliance with other measures (like hand washing…) and inappropriate use of face mask (touching, not washing/changing regularly, incorrect disposal) which may increase risks to themselves and others.
He then identifies other potential side effects to consider include compromised quality/volume of speech, exhaled air goes into eyes (impulse to touch eyes, possibly infect oneself), increased difficulty breathing (increasing frequency and deepness may lead to inhaling more carbon dioxide with each respiratory cycle which may increase viral load for infected people, among other concerns – notes effect amplified if masks heavily contaminated…), innate immunity efficacy depends highly on viral load – if masks determine a humid habitat where virus remains active, an increase in viral load is result and can cause a defeat of innate immunity and increase in infections.
Article oncludes by stating, “we believe that the context of the current covid-19 pandemic is very different from that of the “parachutes for jumping out of aeroplanes”,[7] in which the dynamics of harm and prevention are easy to define and even to quantify without the need of research studies. It is necessary to quantify the complex interactions that may well be operating between positive and negative effects of wearing surgical masks at population level. It is not time to act without evidence.”
MEDICAL REVIEW: Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis (2016)
Read Medical Review — Smith, J.D. et al. (2016) “Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis,” CMAJ Mar 2016
Cliff Notes & Pull Quotes:
This medical review is directly referenced as part of the white paper, “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” as follows: “We identified six clinical studies … . In the meta-analysis of the clinical studies, we found no significant difference between N95 respirators and surgical masks in associated risk of (a) laboratory-confirmed respiratory infection, (b) influenza-like illness, or (c) reported work-place absenteeism.”
RE: all studies/medical reviews cited and discussed in “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” the following general conclusion is drawn (in addition to otherwise going into many aspects worth reading):
“Conclusion Regarding That Masks Do Not Work
No RCT study with verified outcome shows a benefit for HCW or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions.
Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
Masks and respirators do not work.”
MEDICAL ARTICLE: Do facemasks protect against COVID‐19? (6/16/2020)
Pull Quotes:
“The public might wear masks to avoid infection or to protect others. During the 2009 pandemic of H1N1 influenza (swine flu), encouraging the public to wash their hands reduced the incidence of infection significantly whereas wearing facemasks did not. 5 There is no good evidence that facemasks protect the public against infection with respiratory viruses, including COVID‐19. 6”
“However, absence of proof of an effect is not the same as proof of absence of an effect. During the pandemics caused by swine flu and by the coronaviruses which caused SARS and MERS, many people in Asia and elsewhere walked around wearing surgical or homemade cotton masks to protect themselves. One danger of doing this is the illusion of protection. [emphasis added] Surgical facemasks are designed to be discarded after single use. As they become moist they become porous and no longer protect. [emphasis added] Indeed, experiments have shown that surgical and cotton masks do not trap the SARS‐CoV‐2 (COVID‐19) virus, which can be detected on the outer surface of the masks for up to 7 days. 7 , 8 Thus, a pre‐symptomatic or mildly infected person wearing a facemask for hours without changing it and without washing hands every time they touched the mask could paradoxically increase the risk of infecting others. [emphasis added] Because the USA is in a desperate situation, their Centers for Disease Control has recommended the public wear homemade cloth masks. This was essentially done in an effort to try and reduce community transmission, especially from people who may not perceive themselves to be symptomatic, rather than to protect the wearer, although the evidence for this is scant. In contrast, the World Health Organization currently recommends against the public routinely wearing facemasks.”

MEDICAL REVIEW: The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence (2012)
Read Review — bin-Reza et al. (2012) “The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence,” Influenza and Other Respiratory Viruses 6(4), 257–267.
Cliff Notes & Pull Quotes:
This medical review is directly referenced as part of the white paper, “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” as follows: “There were 17 eligible studies. … None of the studies established a conclusive relationship between mask/respirator use and protection against influenza infection.”
RE: all studies/medical reviews cited and discussed in “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” the following general conclusion is drawn (in addition to otherwise going into many aspects worth reading):
“Conclusion Regarding That Masks Do Not Work
No RCT study with verified outcome shows a benefit for HCW or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions.
Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
Masks and respirators do not work.”
MEDICAL REVIEW: Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis (2020)
Read Medical Review — Long, Y. et al. (2020) “Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis,” J Evid Based Med. 2020; 1- 9.
Cliff Notes & Pull Quotes:
This medical review is directly referenced as part of the white paper, “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” as follows: “A total of six RCTs involving 9,171 participants were included. There were no statistically significant differences in preventing laboratory-confirmed influenza, laboratory-confirmed respiratory viral infections, laboratory-confirmed respiratory infection, and influenza-like illness using N95 respirators and surgical masks. Meta-analysis indicated a protective effect of N95 respirators against laboratory-confirmed bacterial colonization (RR = 0.58, 95% CI 0.43-0.78). The use of N95 respirators compared with surgical masks is not associated with a lower risk of laboratory-confirmed influenza.”
RE: all studies/medical reviews cited and discussed in “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” the following general conclusion is drawn (in addition to otherwise going into many aspects worth reading):
“Conclusion Regarding That Masks Do Not Work
No RCT study with verified outcome shows a benefit for HCW or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions.
Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
Masks and respirators do not work.”
MEDICAL OPINION: Universal Masking in Hospitals in the Covid-19 Era (5/21/2020)
Cliff Notes & Pull Quotes:
This feature was written in response to conditions in May 2020 that had “frontline providers are wondering whether this effort should include universal use of masks by all health care workers.”
It states:
1) “We know that wearing a mask outside health care facilities offers little, if any, protection from infection…”
2) “The chance of catching Covid-19 from a passing interaction in a public space is…minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.”
3) The calculus may be different, however, in health care settings…There are two scenarios in which there may be possible benefits…The first is during the care of a patient with unrecognized Covid-19. A mask alone in this setting will reduce risk only slightly, however, since it does not provide protection from droplets that may enter the eyes or from fomites on the patient or in the environment that providers may pick up on their hands and carry to their mucous membranes (particularly given the concern that mask wearers may have an increased tendency to touch their faces)…[second is related to…] instances in which staff members either came to work well but developed symptoms of Covid-19 partway through their shifts or worked with mild and ambiguous symptoms that were subsequently diagnosed as Covid-19…”
4) “…universal masking alone is not a panacea. A mask will not protect providers caring for a patient with active Covid-19 if it’s not accompanied by meticulous hand hygiene, eye protection, gloves, and a gown. A mask alone will not prevent health care workers with early Covid-19 from contaminating their hands and spreading the virus to patients and colleagues. Focusing on universal masking alone may, paradoxically, lead to more transmission of Covid-19 if it diverts attention from implementing more fundamental infection-control measures.
5) “The extent of marginal benefit of universal masking over and above these foundational measures is debatable…the prevalence of Covid-19 among asymptomatic evacuees from Wuhan during the height of the epidemic there was only 1 to 3%.“
6) “Expanded masking protocols’ greatest contribution may be to reduce the transmission of anxiety, over and above whatever role they may play in reducing transmission of Covid-19.”
CDC Related & Medical Studies…
Mask study published by NIH suggests N95 Covid masks may expose wearers to dangerous level of toxic compounds linked to seizures and cancer (8/27/23)
Cliff Notes & Pull Quotes:
NIH re-shared study suggesting N95 masks “may expose users to dangerous levels of toxic chemicals.”
Researchers looked at disposable, medical-grade masks and cotton masks.
Key Points:
- “The study found that the chemicals released by these masks had eight times the recommended safety limit of toxic volatile organic compounds (TVOCs)”
- “Inhaling TVOCs has been linked to health issues like headaches and nausea, while prolonged and repeated has been linked to organ damage and even cancer.”
- An April study found “several disposable masks contain more than eight times the US recommended limit of toxic volatile organic compounds (TVOCs)”
The remainder of the article discusses aspects of various opinions while also pointing to the following facts in reference to the above study:
- “The disposable masks contained up to 14 times the TVOCs than cotton masks”
- “The Environmental Protection Agency (EPA) recommends keeping TVOC levels below 0.5 parts per million in indoor air”
- “The sample with the highest amount of TVOCs had 4,808 cubic meters per microgram, which is about 4.8 parts per million” (more than 8 times recommended limit)
Read full article here: https://www.dailymail.co.uk/health/article-12443319/Mask-study-published-NIH-suggests-N95-Covid-masks-expose-wearers-dangerous-level-toxic-compounds-linked-seizures-cancer.html
Not Even N95 Masks Work To Stop Covid (12/1/2022)
Cliff Notes & Pull Quotes:
This feature compares statements made by policy makers re: effectiveness of masks to support their policies and another extremely high quality, random controlled trial (RCT) study that compared “ability of medical masks to prevent COVID infection to fit-tested N95s” and resulted in demonstrating that masks are “ineffective, regardless off type.”
Study was:
- conducted on healthcare workers (fit-tested, used to using masks appropriately…)
- designed to see if N95s were superior to “regular” surgical masks
- looked at 29 different facilities around the world
- tracked percentage of HC workers testing positive to evaluate infection prevention
- conclusive: zero difference between surgical or N95 respirators as relates to test results
To read more about this study in detail go here: https://brownstone.org/articles/not-even-n95-masks-work-to-stop-covid/
Despite such studies, the media continues to report the opposite…one example four days AFTER the above feature appeared is as follows:

Scientists Studied 12 Masks — Every One Contained This Cancer-Causing Compound (11/03/2022)
Cliff Notes & Pull Quotes:
This feature by Dr. Joseph Mercola cites a study of 12 face masks that showed “every mask contained titanium dioxide (Ti02) particles in at least one layer, at levels that “exceeded the acceptable exposure level.”
It notes that:
- The International Agency for Research on Cancer classifies titanium dioxide as a “Group 2B carcinogen), meaning “possibly carcinogenic to humans” when inhaled
- Meta-analysis cites numerous toxic effects of titanium dioxide in humans and aquatic animals and calls for a “rethinking of nano-Ti02” safety
- Physical and psychological toll of masks includes emotional burdens highlighted in journal Pediatrics
- YouTube has changed policy to now allow saying masks don’t work
To read about these and many more compelling facts in this article go to https://childrenshealthdefense.org/defender/masks-titanium-dioxide-cancer-cola/
What studies/literature reviews does CDC LIST to support its GUIDELINES for universal masking? Does anyone read them?
Cliff Notes & Pull Quotes:
First, the CDC references 10 randomized controlled trials, concluding:
(1) “In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks…”
(2) “Disposable medical masks (also known as surgical masks)… our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza”
(3) Otherwise CDC notes it disregarded evaluation of respirators (N95 and the like) and cited known complications between “theory” vs. “reality,” as regards cloth masks.
Second, the CDC website lists the following “recent studies” [in support of universal masking], concluding:
(1) Rothe C, Schunk M, Sothmann P, et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. The New England journal of medicine. 2020;382(10):970-971. What is this study about? Found here, this study focuses on a single individual and (3) others with whom this person came into contact, concludes, “the viability of 2019-nCoV detected on qRT-PCR in this patient remains to be proved by means of viral culture.” and makes NO mention of masks whatsoever.
(2) Zou L, Ruan F, Huang M, et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. The New England journal of medicine. 2020;382(12):1177-1179. What is this study about? Found here, this study references 18 patients regarding topic of viral loads, concludes, “we need better data to determine transmission dynamics and inform our screening practices” and makes NO mention of masks whatsoever.
(3) Pan X, Chen D, Xia Y, et al. Asymptomatic cases in a family cluster with SARS-CoV-2 infection. The Lancet Infectious diseases. 2020. What is this study about? Found here or in The Lancet here, this study focuses on (1) 3-member family, concludes, “more studies are needed to observe the symptoms and test results of infected individuals in greater detail” and makes NO mention of masks whatsoever.
(4) Bai Y, Yao L, Wei T, et al. Presumed Asymptomatic Carrier Transmission of COVID-19. Jama. 2020. What is this study about? Found here, this study focuses on possible transmission from an asymptomatic Wuhan resident to 5 family members in another province, concludes, “If the findings in this report…are replicated, the prevention of COVID-19 infection would prove challenging. The mechanism by which asymptomatic carriers could acquire and transmit the coronavirus that causes COVID-19 requires further study” and makes NO mention of masks whatsoever.
(5) Kimball A HK, Arons M, et al. Asymptomatic and Presymptomatic SARS-CoV-2 Infections in Residents of a Long-Term Care Skilled Nursing Facility — King County, Washington, March 2020. MMWR Morbidity and mortality weekly report. 2020; ePub: 27 March 2020. What is this study about? Found here, this study focuses on testing residents of a long-term care facility in Washington state, concludes, “Long-term care facilities should take proactive steps to prevent introduction of SARS-CoV-2 (3). Once a confirmed case is identified… all residents should be placed on isolation precautions… with considerations for extended use or reuse of personal protective equipment (PPE) as needed (4).” Aside from this last note that refers to coping with PPE shortages, this study otherwise makes NO mention of masks whatsoever.
(6) Wei WE LZ, Chiew CJ, Yong SE, Toh MP, Lee VJ. Presymptomatic Transmission of SARS-CoV-2 — Singapore, January 23–March 16, 2020. MMWR Morbidity and Mortality Weekly Report. 2020;ePub: 1 April 2020. What is this study about? Found here, this study reviewed 243 confirmed cases, identified (7) clusters of cases in which presymptomatic transmission likely occurred, concluded, “…it might not be enough for only persons with symptoms to limit their contact with others because persons without symptoms might transmit infection,” emphasized social distancing and otherwise makes NO mention of masks whatsoever.
(7) Li R, Pei S, Chen B, et al. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science (New York, NY). 2020. What is this study about? Found here, this study analyzed data from Tencent “with a networked dynamic metapopulation model and Bayesian inference” to analyze early spread within China, concluded, “…findings indicate that a large proportion of COVID-19 infections were undocumented prior to the implementation of travel restrictions and other heightened control measures…and that a large proportion of the total force of infection was mediated through these undocumented infections” and “…awareness among health care providers and public health officials and the availability of viral identification assays suggest that capacity for identifying previously missed infections has increased” and “general population and government response efforts have increased the use of face masks, restricted travel, delayed school reopening, and isolated suspected persons, all of which could [emphasis added additionally slow the spread of SARS-CoV-2″ and, other than tangential reference such as this, masks were not evaluated for efficacy whatsoever by this study.
(8) Furukawa NW, Brooks JT, Sobel J. Evidence Supporting Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 While Presymptomatic or Asymptomatic [published online ahead of print, 2020 May 4]. Emerg Infect Dis. 2020;26(7):10.3201/ eid2607.201595. What is this study about? Found here, this feature searched literature for evidence supporting presymptomatic and asymptomatic transmission up until the point when CDC “made policy changes recommending community cloth face coverings and universal masking in healthcare facilities” and states, “…knowing that asymptomatic transmission was a possibility, CDC recommended key interventions including physical distancing (36), use of cloth face coverings in public (37), and universal masking in healthcare facilities (38) to prevent SARS-CoV-2 transmission by asymptomatic and symptomatic persons with SARS-CoV-2 infection.” These are the only references to universal masking in this article. As such, we reviewed the (2) studies related to masks that are listed as part of the review material included and found:
(a) The first one, here, reviewed evidence re: cloth masks. One item reviewed notes that healthcare workers, “..should not use cloth masks as protection against respiratory infection. Cloth masks resulted in significantly higher rates of infection than medical masks, and also performed worse than the control arm” [emphasis added] and another states, ““The evidence is not sufficiently strong to support widespread use of facemasks as a protective measure against covid-19. However, there is enough evidence to support the use of facemasks for short periods of time by particularly vulnerable individuals when in transient higher risk situations.” The article goes into more discourse before noting the following statement made by the WHO, “…there is currently no evidence that wearing a mask (whether medical or other types) by healthy persons in the wider community setting, including universal community masking, can prevent them from infection with respiratory viruses, including covid-19. Wearing masks in the community can also give people a false sense of security, it said, and lead to them neglecting other measures, such as hand hygiene and physical distancing” [emphasis added] and, ultimately, providing no conclusive evidence of any real efficacy of universal masking.
(b) The second one here focuses on use of masks in hospital settings and notes, “We know that wearing a mask outside health care facilities offers little, if any, protection from infection” [emphasis added] and states, “…a mask will not protect providers caring for a patient with active Covid-19 if it’s not accompanied by meticulous hand hygiene, eye protection, gloves, and a gown. A mask alone will not prevent health care workers with early Covid-19 from contaminating their hands and spreading the virus to patients and colleagues. Focusing on universal masking alone may, paradoxically, lead to more transmission of Covid-19 if it diverts attention from implementing more fundamental infection-control measures.” [emphasis added] This study also notes curious benefits of universal masking include, “Masks are visible reminders of an otherwise invisible yet widely prevalent pathogen and may remind people of the importance of social distancing and other infection-control measures” and “masks serve symbolic roles. Masks are not only tools, they are also talismans that may help increase health care workers’ perceived sense of safety, well-being, and trust in their hospitals….expanded masking protocols’ greatest contribution may be to reduce the transmission of anxiety, over and above whatever role they may play in reducing transmission of Covid-19.” Note, while admitting to the ineffective nature of masks to prevent transmission outside the hospital setting, this study offers absolutely no proof of any efficacy of universal masking whatsoever.
(9) Oran DP, Topol Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review [published online ahead of print, 2020 Jun 3]. Ann Intern Med. 2020;M20-3012. What is this study about? Found here, this is a review and synthesis of available evidence on asymptomatic SARS-CoV-2 infection. It admits, “Most data from the 16 cohorts in this narrative review are not the output of large, carefully designed studies with randomly selected, representative samples…” and so declare, “…these data may offer potentially valuable insights into SARS-CoV-2 incidence and the highly variable effect of infection.” Essentially, this is not a review of Random Controlled Trials which leads to much use of language typical of hypothesis (“may,” “could,” “likely,” etc.). After review of all items, it recommends “innovative surveillance tactics” for “public health surveillance” to overcome challenges in obtaining “useful data for public health officials” and specifically mentions such things as “self monitoring with internet-connected thermometers and smart watches that monitor heart rate: and “crowdsourcing the resulting data” and “monitoring sewage sludge.” This study makes one tangential reference to masks with regard to one item under review but otherwise offers absolutely no proof of any efficacy of universal masking whatsoever.
(10) National Academies of Sciences, Engineering, and Medicine. 2020. Rapid Expert Consultation on the Possibility of Bioaerosol Spread of SARS-CoV-2 for the COVID-19 Pandemic (April 1, 2020). Washington, DC: The National Academies Press. What is this consultation about? Found here, this paper focuses on mode of transmission. The only reference to universal masking was in regard to, “Leung et al. 2020. Respiratory virus shedding in exhaled breath and efficacy of face masks” that is detailed in item (17) below and includes the following results: “among the samples collected without a face mask, we found that the majority of participants with influenza virus and coronavirus infection did not shed detectable virus in respiratory droplets or aerosols.” and “For those who did shed virus in respiratory droplets and aerosols, viral load in both tended to be low…and given that each exhaled breath collection was conducted for 30 min, this might imply that prolonged close contact would be required for transmission to occur, even if transmission was primarily via aerosols.” Under limitations, it notes, “The major limitation of our study was the large proportion of participants with undetectable viral shedding in exhaled breath for each of the viruses studied. We could have increased the sampling duration beyond 30 min to increase the viral shedding being captured, at the cost of acceptability in some participants. An alternative approach would be to invite participants to perform forced coughs during exhaled breath collection12.“
(11) Schwartz KL, Murti M, Finkelstein M, et al. Lack of COVID-19 transmission on an international flight. CMAJ. 2020;192(15):E410. What is this feature about? Found here, this document provides details re: public health response to the first Canadian cases of coronavirus disease 2019 (COVID-19) – an “index” patient and his wife who were part of a 350 passenger flight from Wuhan to Canada. As a result of such nominal transmission found, this case study suggests, “transmission may have been mitigated by mild symptoms and masking during the flight. However, the lack of secondary cases after prolonged air travel exposure supports droplet transmission, not airborne, as the likely route of spread…” This feature does not clarify to what extent anyone may have been masked during the flight and otherwise offers absolutely no proof of any efficacy of universal masking whatsoever.
(12) Anfinrud P, Stadnytskyi V, Bax CE, Bax A. Visualizing Speech-Generated Oral Fluid Droplets with Laser Light Scattering. N Engl J Med. 2020 Apr 15. doi:10.1056/NEJMc2007800. What is this letter about? Found here, because “aerosols and droplets generated during speech have been implicated in the person-to-person transmission of viruses,” this letter reports results of “a laser light-scattering experiment in which speech-generated droplets and their trajectories were visualized.” Although this letter refers to study of a person speaking “with and without a face mask,” it references using a damp washcloth over the speaker’s mouth, which “showed a decrease in the number of forward-moving droplets.” It is unclear how this experiment serves to demonstrate efficacy of face masks re: transmission as this experiment did not assesss “the relative roles of droplets of droplets generated during speech, droplet nuclei,2 and aerosols in the transmission of viruses” but sought only “to provide visual evidence of speech-generated droplets and to qualitatively describe the effect of a damp cloth cover over the mouth to curb the emission of droplets.”
(13) Davies A, Thompson KA, Giri K, Kafatos G, Walker J, Bennett A. Testing the efficacy of homemade masks: would they protect in an influenza pandemic? Disaster Med Public Health Prep. 2013;7(4):413-8. What was this study about? Found here, this study focused on (21) healthy volunteers who made face masks from cotton t-shirts and which were tested for fit. Volunteers “coughed twice into the box, and the air inside was sampled for 5 minutes. Each volunteer was sampled 3 times: wearing the homemade mask, the surgical mask, and no mask.” Results note, “The number of microorganisms isolated from the coughs of healthy volunteers was generally low, although this varied according to the individual sampled (Table 3). It is possible, therefore, that the sampling limitations negatively affected the statistical analysis” and ” if as a mask it does not fit well around the nose and mouth, or the material freely allows infectious aerosols to pass through it, then it will be of no benefit.” It concludes, “A protective mask may reduce the likelihood of infection, but it will not eliminate the risk…any mask, no matter how efficient at filtration or how good the seal, will have minimal effect if it is not used in conjunction with other preventative measures, such as isolation of infected cases, immunization, good respiratory etiquette, and regular hand hygiene. An improvised face mask should be viewed as the last possible alternative if a supply of commercial face masks is not available, irrespective of the disease against which it may be required for protection. Improvised homemade face masks may be used to help protect those who could potentially, for example, be at occupational risk from close or frequent contact with symptomatic patients. However, these masks would provide the wearers little protection from microorganisms from others persons who are infected with respiratory diseases. As a result, we would not recommend the use of homemade face masks as a method of reducing transmission of infection from aerosols.”
(14) Konda A, Prakash A, Moss GA, Schmoldt M, Grant GD, Guha S. Aerosol Filtration Efficiency of Common Fabrics Used in Respiratory Cloth Masks. ACS Nano. 2020 Apr 24. What is this study about? Found here, this paper reports “results of experiments where we measure the filtration efficiencies of a number [15] of common fabrics, as well as selective combinations for use as hybrid cloth masks, as a function of aerosol sizes ranging from ∼10 nm to 6 μm” noting, “…aerosols remain suspended in the air for longer durations due to their small size and play a key role in spreading infection.” [they note: SARS-CoV-2 virus has been shown to remain suspended in air for ~3 h.] They point out the importance of fit (that leads to gaps) while using the face mask” and note that, “the effect of gaps between the contour of the face and the mask as caused by an improper fit will affect the efficiency of any face mask.21,27,28,33 This is of particular relevance to cloth and surgical masks that are used by the public and which are generally not “fitted”, unlike N95 masks or elastomeric respirators.” Particles evaluated were “in the significant (for aerosol-based virus transmission) size range of ∼10 nm to ∼6 μm” and findings included that “cotton, natural silk, and chiffon can provide good protection, typically above 50% in the entire 10 nm to 6.0 μm range, provided they have a tight weave. Higher threads per inch cotton with tighter weaves resulted in better filtration efficiencies…Our findings indicate that leakages around the mask area can degrade efficiencies by ∼50% or more, pointing out the importance of “fit”…in summary, we find that the use of cloth masks can potentially provide significant protection against the transmission of particles in the aerosol size range.”
(15) Aydin O, Emon B, Saif MTA. Performance of fabrics for home-made masks against spread of respiratory infection through droplets: a quantitative mechanistic study. medRxiv posted April 24, 2020.
Found here, this study reports repiratory infections “may spread through droplets and aerosols released by infected individuals coughing, sneezing, or speaking” and asserts focus, “How effective cloth face coverings can be at reducing transmission via large droplets therefore remains elusive.”
This study looked at how 11 household fabrics performed “at blocking high-velocity droplets.” Other factors assessed included, “breathability (air permeability), texture, fiber composition, and water absorption properties” and a commercial medical mask was used as a “benchmark.”
They loaded the nozzle of an inhaler with flourescent nanoparticles (beads) in distilled water to mimic SARS-CoV-2 virus partiles carried by water. The internal pressure of the inhaler when pressed ejected it, creating “high-speed droplets” that then hit teh sample fabric placed in front of the inhaler.
Note, this study declares, “Established knowledge from aerosol science may not be immediately applicable to determine the efficiency of mask materials at blocking larger droplets carrying virus particles.” Given that A) previous research indicates that the SARS-CoV-2 virus is subject to aerosol transmission and B) it is common scientific knowledge that masks may help slow forward transmission, however do not prevent aersoloized particles from exiting from the top, bottom, sides and even forward, through masks [so not merely forward as with this study using an inhaler] and even this study notes, “medical masks or cloth face coverings typically cannot ensure tight sealing against the contours of the face. As a result, a significant portion of the air released during breathing, sneezing, and coughing may escape through the gaps, potentially carrying some of the respiratory droplets with virus particles with it“ C) the CDC recently acknowledged and then withdrew its acknowledgement that the virus is transmitted via aerosols and D) the CDC now has done another 180 and affirmed that transmission occurs via aerosols, this declaration raises questions of applicability re: real-world transmission that is acknowledged to occur both via droplets and aerosols.
That said, the study found the less breathable the fabrics, the more effective at blocking droplets: “Our measurements indicate that 2 or 3 layers of highly permeable fabric, such as T-shirt cloth, may block droplets with an efficacy similar to that of medical masks, while still maintaining comparable breathability.”
Results suggest cloth face coverings “may” help reduce droplet transmission and note “biodegradable fabrics such as cotton allow washing and reusing, and can help reduce the adverse environmental effects of widespread use of commercial disposable and non-biodegradable facemasks.”
(16) Ma QX, Shan H, Zhang HL, Li GM, Yang RM, Chen JM. Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. J Med Virol. 2020.
Study, found here, evaluates efficacy of (3) types of masks (see below) and instant hand wiping, using avian influenza for test. Results showed instant hand wiping “…removed 98.36%, %, 96.62%, and 99.98% of the virus from hands, respectively.”
In lieu of researching real-world conditions, this study set up lab conditions to simulate by using a nebulizer where the top parts of syringes “were removed and then wrapped with the tested masks” which were, respectively, a) homemade mask of polyester cloth plus 4-layers of kitchen paper [towels], and b) a medical mask and c) an N95 mask. “QVS facial cleaning sponge…made of hydrophilic polyvinyl alcohol was set inside the syringe behind the mask…for collecting the virus passing through the masks. The four syringes were then aligned and bound seamlessly together.”
Results of this method found all three masks “could block 99.98%, 97.14%, and 95.15% of the virus in aerosols” and the authors suggest masks and hand washing “to slow the exponential spread of the virus.”
(17) Leung, N.H.L., Chu, D.K.W., Shiu, E.Y.C. et al.Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. 2020. What is this study about? Found here, this study explores respiratory droplet and aerosol routes of transmission specifically for coronaviruses, influenza viruses and rhinoviruses “by quantifying the amount of respiratory virus in exhaled breath of participants with medically attended ARIs and determining the potential efficacy of surgical face masks to prevent respiratory virus transmission.” Results include, “…aerosol transmission is a potential mode of transmission for coronaviruses as well as influenza viruses and rhinoviruses” and “our findings indicate that surgical masks can efficaciously reduce the emission of influenza virus particles into the environment in respiratory droplets, but not in aerosols12.” It also suggests there are “…important implications for control of COVID-19, suggesting that surgical face masks could be used by ill people to reduce onward transmission.” Morover, it states, “among the samples collected without a face mask, we found that the majority of participants with influenza virus and coronavirus infection did not shed detectable virus in respiratory droplets or aerosols.” and “For those who did shed virus in respiratory droplets and aerosols, viral load in both tended to be low…and given that each exhaled breath collection was conducted for 30 min, this might imply that prolonged close contact would be required for transmission to occur, even if transmission was primarily via aerosols.” Finally, it notes, “The major limitation of our study was the large proportion of participants with undetectable viral shedding in exhaled breath for each of the viruses studied. We could have increased the sampling duration beyond 30 min to increase the viral shedding being captured, at the cost of acceptability in some participants. An alternative approach would be to invite participants to perform forced coughs during exhaled breath collection12.“
(18) Johnson DF, Druce JD, Birch C, Grayson ML. A quantitative assessment of the efficacy of surgical and N95 masks to filter influenza virus in patients with acute influenza infection. Clin Infect Dis. 2009 Jul 15;49(2):275-7.
Found here, this study tested the “in vivo efficacy” of N95 and surgical masks “to filter reverse transcription polymerase chain reaction (RT-PCR)-detectable virus when worn correctly by [nine] patients with laboratory-confirmed acute influenza.”Results determined both masks “were equally effective in preventing the spread of PCR-detectable influenza.”
[NOTE: in addition to being a very small sample, it is common knowledge that one of the most significant problems that is a source of risk brought up in so many studies and commentaries on universal masking in community is that people generally do not correctly wear masks; they touch their faces, don’t frequently change/wash masks, etc.]
(19) Green CF, Davidson CS, Panlilio AL, et al. Effectiveness of selected surgical masks in arresting vegetative cells and endospores when worn by simulated contagious patients. Infect Control Hosp Epidemiol. 2012;33(5):487‐494.
Found here, the objective of this study was to quantify the efficacy of “selected surgical masks in arresting vegetative cells and endospores in an experimental model that simulated contagious patients.”
As with previous study listed, this study is not a real-world evaluation but an experiment under lab conditions in which mannequin heads were fitted with surgical masks that had been “retrofitted with a nebulizer attached to an automated breathing simulator” and “Aerosols of endospores or vegetative cells were generated with a modified microbiological research establishment-type 6-jet collision nebulizer, while air samples were taken with all-glass impinger (AGI-30) samplers downstream of the point source. All experiments were conducted in a horizontal bioaerosol chamber.”
Results showed there were “no statistically significant differences in arrestance observed between models of surgical masks challenged with vegetative cells” and that the mean “arrestance of bioaerosols” by the masks were 48-68% for endospores and 66-76% with vegetative cells.
The study concludes that, in the case of “simulated contagious patients” wearing masks is supported as “one of the recommended cough etiquette interventions to limit the transmission of airborne infectious agents.”
NEWS: CDC Study Finds Overwhelming Majority of People Getting Coronavirus Wore Masks (10/12/2020)
Cliff Notes & Pull Quotes:
A September CDC report shows face masks ineffective.
U.S. study found over 70% of the 154 “case patients” (those who tested postive for Covid-19) “were contaminated with the virus and fell ill despite “always” wearing a mask.”
Noted “limitations” of study were cited as follows:
“The findings in this report are subject to at least five limitations. First, the sample included 314 symptomatic patients who actively sought testing during July 1–29, 2020 at 11 health care facilities. Symptomatic adults with negative SARS-CoV-2 test results might have been infected with other respiratory viruses and had similar exposures to persons with cases of such illnesses. Persons who did not respond, or refused to participate, could be systematically different from those who were interviewed for this investigation. Efforts to age- and sex-match participating case-patients and control-participants were not maintained because of participants not meeting the eligibility criteria, refusing to participate, or not responding, and this was accounted for in the analytic approach. Second, unmeasured confounding is possible, such that reported behaviors might represent factors, including concurrently participating in activities where possible exposures could have taken place, that were not included in the analysis or measured in the survey. Of note, the question assessing dining at a restaurant did not distinguish between indoor and outdoor options. In addition, the question about going to a bar or coffee shop did not distinguish between the venues or service delivery methods, which might represent different exposures. Third, adults in the study were from one of 11 participating health care facilities and might not be representative of the United States population. Fourth, participants were aware of their SARS-CoV-2 test results, which could have influenced their responses to questions about community exposures and close contacts. Finally, case or control status might be subject to misclassification because of imperfect sensitivity or specificity of PCR-based testing (9,10).”
[Note: it has elsewhere been asserted that PCR testing can be unreliable as it was not designed/intended to be used for such a purpose as is being implemented in testing for the SARS-Cov-2 virus. Here is at least one article related to the topic: https://mises.org/wire/false-positive-panic-over-covid-19]
STUDY: Cloth Masks - dangerous to your health? (4/22/15)
Cliff Notes & Pull Quotes:
This randomised clinical trial to study the efficacy of cloth masks found “respiratory infection was much higher among healthcare workers wearing cloth masks” and “the penetration of cloth masks by particles was almost 97% compared to medical masks with 44%.”
This study concluded, “Cloth masks should not be used by workers in any healthcare setting, but particularly high-risk situations such as emergency departments, intensive care, paediatric or respiratory wards.”
Authors of this study, “speculate that the cloth masks’ moisture retention, their reuse and poor filtration may explain the increased risk of infection.”

FLIP FLOP FAUCI - NO mask? YES mask? Why is he against performing a controlled study?
Regardless of political affiliation, many can agree that a great deal of conflicting information around the topic of masks has prompted unnecessary confusion, fear and questionable behavior, at best (consider how many people somehow see fit to verbally abuse “essential workers” and/or perfect strangers and even to physically assault people in their community for either not wearing a mask or having it under their nose, perhaps even to gain a moment of unfettered intake of a #1 most essential requirement for all human beings to sustain life…). Some conflicting information has even been provided by Dr. Fauci himself:
(1) Consistent with the great plethora of medical studies available, in an interview with CNN, Dr. Fauci declared that masks do not work: “…there’s no reason to be walking around with a mask. When you’re in the middle of an outbreak, wearing a mask might make people feel a little bit better and it might even block a droplet, but it’s not providing the perfect protectiong that people think that it is. And, often, there are unintended consequences – people keep fiddling with the mask and they keep touching their face…but when you think masks, you should think of healthcare providers needing them and people who are ill.”
(2) Dr. Fauci next testifies that masks DO work but that they simply LIED (notably, he claims the basis for this is that they wanted to keep them available to those [healthcare workers] putting their lives in harm’s way – yet, as others are quick to point out, the whole point of surgical mask-wearing is to protect patients from being sprayed with spit from coughs, sputters and what not, not to protect doctors – yet NOW the claim is that it’s to protect the 1st responders? Also noteworthy is that many who support the notion of universal masking of healthy individuals do so based on the belief that masks protect OTHERS – so which is it? For clarification, here’s a link to at least one doctor’s explanation of this point).
(3) Then, on 7/16/2020, Dr. Fauci expresses his OPPOSITION to doing a controlled study of universal masking of healthy people. The basis for his position? Pull Quote: “…Fauci balked at the idea. “I would not want to do a randomized controlled study because that would mean having people not wear masks and see if they do better,” he said.”
(4) Then, on 7/24/2020, Dr. Fauci watches a baseball game without wearing a mask. But, only a week before he stated that doing a study was too risky because it would involve people not wearing masks – so which is it?
While Americans keep doing their best to follow along, reporters like Tucker Carlson reveal that the CDC revised their own “guidance” to better align with truth / science, stating:”…the CDC acknowledged that researchers lack evidence that – quote – “masks offer any protection against coronavirus.” ANY. At ALL…”
Finally, even more recently, the CDC adjusted its recorded deaths due to Covid-19 downward, revealing that only 6% of reported deaths were actually due TO Covid.
CDC announces cloth masks ineffective against particles even larger than the virus(9/11/2020)
Cliff Notes & Pull Quotes:
@AlexBerenson retweets a CDC announcement, adding commentary of his own. He writes:
VIDEO: Dennis Prager: May CDC Study: Masks Could Actually Increase Risk of Virus Transmission (7/21/2020)
Cliff Notes and Pull Quotes:
Dennis Prager discusses a CDC study from May 2020 that shows how ineffectual masks and even handwashing are, including how masks could increase risk of virus transmission.
Video opens with commentary re: cost to society related to veiling its population; making people invisible; dehumanizing.
Just after 3:20 mark, Mr. Prager reads from the study, “Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures.
Key takeaways: “According to the study: “In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks,” and additionally, “improper use might increase the risk for transmission.”
NEWS: CDC guidelines say wearing a mask during prolonged exposure to coronavirus won't prevent possible infection (8/24/2020)
Cliff Notes & Pull Quotes:
Feature opens: “Guidelines from the Centers for Disease Control and Prevention state that those who come in close contact with someone with the coronavirus for more than 15 minutes could spread the virus regardless of whether either party wears a mask.
“Wondering what @cdcgov really thinks about masks? Their guidance on quarantining after exposure to someone with #covid explicitly states whether the infected OR exposed person wore masks doesn’t matter,” former New York Times reporter Alex Berenson tweeted Sunday [8/23/2020].
“My mask protects no one. So does yours. Thanks for clearing that up, CDC!” he added, accompanied by screenshots of the CDC’s guidelines.”
Feature cites conflicting advice from Dr. Fauci and CDC and notes, “The CDC released a meta-analysis in May 2020 of 14 controlled, extended trials studying the effects of mask usage. The study found no reduction in the rate of laboratory-confirmed cases of influenza, a similar respiratory illness.”
Feature closes with reference to ;eading Swedish epidemiologist, Dr. Anders Tegnell, who dismissed reliance upon masks stating, “I’m surprised that we don’t have more or better studies showing what effect masks actually have. Countries such as Spain and Belgium have made their populations wear masks, but their infection numbers have still risen. The belief that masks can solve our problem is, in any case, very dangerous.”
VIDEO: Tucker Carlson -- CDC ADMITS -- lack of evidence masks are effective - at all... (8/24/2020)
Can surgical masks protect you from getting the flu? (10/17/19)
Cliff Notes & Pull Quotes:
Published prior to 2020, this article features “pre-politicized” information of scientific and common knowledge nature, regarding wearing face masks as preventative measure.
It notes:
1) “Surgical masks are sometimes referred to as courtesy masks…” and “The logic of wearing a surgical mask must surely be: if it works for surgeons, it must work for me. The problem is, the mask isn’t intended to protect the surgeon. It’s intended to stop droplets from the surgeon’s mouth or nose getting into the patient’s wound and causing sepsis. But despite their use for more than a century, their prophylactic effectiveness is in doubt. Indeed, a recent study showed that surgical masks can be a source of bacterial contamination in the operating theatre.”
2) the idea of wearing masks to stop getting the flu relies on the intention of “stopping your hand touching your mouth or nose” while noting, “…one weak point in this plan: you can also get the flu from touching your eye with your contaminated hand. And even to stop the hand to mouth/nose transmission, you’d have to wear a mask 24/7, regularly disposing of the old ones while trying to avoid touching your face.“
3) Transmission of influenza virus occurs not only from inhaling droplets, “you can also get the flu from touching anything with the flu virus on it – the armrests on public transport, say – and then touching your face. And people touch their faces a lot without even realising it. A study from New South Wales found that people touch their faces about 23 times an hour.“
4) Discomfort and making communication difficult are other problems associated with wearing face masks, making them an impractical true remedy, “One study found that only 21% of people are able to keep masks on for the recommended time.“
The article visits a common study used to advocate for mask use and it’s significant problematic findings that render it useless to that end.
It concludes, “Basically, there is no strong evidence to support well people wearing surgical masks in public. Or as the US Centers for Disease Control and Prevention put it: “No recommendation can be made at this time for mask use in the community by asymptomatic persons, including those at high risk for complications, to prevent exposure to influenza viruses.” The best thing you can do to stop getting the flu is to regularly wash your hands, and try to avoid touching your face.”

VIDEO: Michelle Malkin -- The Revolt Against Mask Mandates (9/20/2020)
Cliff Notes & Pull Quotes:
Michelle Malkin opens with, “The statue of liberty famously welcomes the huddled masses from around the world yearning to breath free…” and then comments on the unnatural conditions being placed upon Americans due to “manufactured fear.”
By way of video snippets, Malkin next reminds viewers of the exact testimony of leading experts from mere months ago – statements from Dr. Redfield (CDC) before the Foreign Affairs Committee to Dr. Fauci in an interview aired by CBS to Dr. Birx in a press conference stating, “…so we don’t want people to feel like, ‘oh, I’m wearing a mask – I’m protected and I’m protecting others...” to the U.S. Surgeon General via Twitter and more) that each declared masks to be unnecessary, inappropriate and/or ineffective in response to Covid-19 / the pandemic.
Malkin then says it’s hard to believe where we are now and provides the latest video testimony from Dr. Redfield (CDC) that entirely contradicts his previous testimony as he now states, “face masks are the most important powerful public health tool we have…” He also now claims we have clear scientific evidence they work and are our best defense. [Note: now may be a good time to review our toggle titled, “What studies/literature reviews does CDC LIST to support its GUIDELINES for universal masking? Are they hoping nobody actually reads them?”]
After declaring that these hypocritical folks have zero credibility and therefore should have zero power over our lives, Malkin asserts that there is no scientific basis for universal mask mandates and presents the evidence via direct quotes from leading authorities that include:
— OSHA (“Wearing cloth masks will not protect wearers from airborne transmissable infection agents.“)
— European Centre For Disease Prevention and Control (“There is no evidence that non-medical face masks…are an effective means of respiratory protection for the wearer…”)
— Annals of Internal Medicine (“Neither surgical nor cotton masks effectively filtered COVID during coughs by infected patients.”)
— WHO (“There is no direct evidence on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including Covid-19.”)
Malkin then notes that anti-mask mandates movement is gaining steam. She plays a video of a parent at a South Dakota school board meeting being arrested for not wearing a mask, a video of Florida residents taking a stand at their local Target store and a now viral video of elderly people in a nursing home staging a protest of their own. Finally, she notes that a Federal Judge in Pennsylvania struck down the Governor’s mask mandate and other health orders as violations of the First and Fourteenth Amendments. She notes the many lawsuits now being launched in many states, across the country. Malkin closes with the statement that “Informed citizens agree that universal mask mandates are unscientific, unlawful and un-American. Common sense and Constitutional principles, now more than ever, are vital to a sovereign nation’s health.“
CDC UPDATE: CDC: Face masks with vents, valves don't prevent spread of coronavirus (8/13/2020)
Cliff Notes & Pull Quotes:
Now the CDC says face masks with vents or valves do NOT prevent the spread of coronavirus.
“In health guidance issued last week, the CDC quietly announced that such masks can, in fact, increase the amount of “expelled respiratory droplets that can reach others.”
The guidance reads, “The purpose of masks is to keep respiratory droplets from reaching others to aid with source control. However, masks with one-way valves or vents allow air to be exhaled through a hole in the material, which can result in expelled respiratory droplets that can reach others.”
“This type of mask does not prevent the person wearing the mask from transmitting COVID-19 to others,” the guidance adds. “Therefore, the CDC does not recommend using masks for source control if they have an exhalation valve or vent.”
NEWS: CDC Director Ripped Over Claim On Mask Effectiveness: ‘Does He Expect People To Believe That?’ (9/17/2020
Pull Quotes & Cliff Notes:
Critics slam Robert Redfield (director of CDC) after testifying Wednesday before the Senate that face masks may be more effective than a vaccine.
Brit Hume (Senior political analyst at Fox News) questioned the idea masks can protect the wearer from the virus as it has previously been promoted as protection to others, should wearer be infected, say8ing, “For months we’ve been told we should wear masks not so much to protect ourselves as to protect others. Now the head of the CDC is claiming that a mask will protect the wearer better than a vaccine. Does he expect people to believe that?”
The feature criticizes Redfield’s comments as “another twist in health officials evolving recommendations,” reminding readers of the statement made in a Twitter message by Jerome Adams (U.S. Surgeon General), “Seriously people — STOP BUYING MASKS! They are NOT effective in preventing general public from catching #Coronavirus…”
Finally, this feature reminds readers that Dr. Fauci “admitted in June that health officials were not upfront with the America people over the effectiveness of masks” before completely contradicting his own expert opinion that masks are ineffective against Covid-19 / pandemic.
[Note: now might be a good time to see toggle on this page titled, “FLIP FLOP FAUCI – NO mask? YES mask? Why is he against performing a controlled study?”]
Dr. Quack? CDC's Redfield Claims Masks "Guaranteed To Protect Against COVID" (9/17/2020)
Cliff Notes:
This editorial features commentarie from a number of sources (that include video clips, quotes and other direct references) in regards to now conflicting statements by director of CDC, Dr. Redfield.
Redfield’s recent commentary stands in direct conflict with previous statements he has madewith regard to efficacy of masks, as relates to universal masking.
Pull Quotes:
In the February hearing, Redfield advised against Americans buying medical grade masks stating there is “no role for these masks in the community.”
“There remains zero evidence that cloth masks or the earloop masks displayed by Redfield helps to slow the spread of COVID-19 or protect the wearer from infection. No country in the world has proven a link in slowing or stopping the spread due to mask wearing mandates, which are in effect in countless nations.”
VIDEO: Laura Ingraham questions experts and science on masks helping to slow the spread of coronavirus (7/15/2020)
Cliff Notes & Pull Quotes:
Laura Ingram opens with, “Now I want to make clear, I’m not telling anyone not to wear a mask. That’s not what we’re here for. Instead I want to move behind hyperbole and focus on what the latest science actually tells us.”
Ingram notes we’ve heard for months that wearing face masks is a selfless and even patriotic thing to do, which she says sounds pretty cool and even like a unifying thing.
While this is the emotional argument, what about the actual data?
Ingram first reviews an April 2015 study that examined benefits of cloth mask use in healthcare setting and concluded, “The rates of all infection outcomes were highest in the cloth mask arm…Penetration of masks by particles was almost 97% and surgical masks 44%.” Ingram also notes, “The results caution against the use of cloth masks…” [Note: please see toggle titled, “STUDY: A cluster randomised trial of cloth masks compared with medical masks in healthcare workers (4/22/15)]
Ingram next cites the WHO’s (6/5/2020) statement of “ADVICE ON THE USE OF MASKS IN THE CONTEXT OF COVID-19” which clarifies, “There is limited evidence that wearing a medical mask by healthy individuals in households, in particular those who share a house with a sick person, or among attendees of mass gatherings may be beneficial as a measure preventing transmission…At present, there is no direct evidence…of the effectiveness…of universal masking of healthy people in the community to prevent infection of respiratory viruses, including Covid-19.”
Next, Ingram cites the “gold standard itself – the CDC,” reminding viewers it recommended against masks in January and that Dr. Fauci repeated this guidance (a video clip of his comments that can be found on this page under toggle titled, “FLIP FLOP FAUCI – NO mask? YES mask? Why is he against performing a controlled study?” is played). Ingram also notes that Facebook now flags his old interview as “false information.”
Ingram next provides results from a study published in Nature (5/27/2020) that compared viral shedding of coughing by infected patients is consistent with Fauci’s original statement and concludes, “among the samples collected without a face mask, we found that the majority of participants with influenza virus and coronavirus infection did not shed detectable virus in respiratory droplets or aerosols…for those who did shed virus in respiratory droplets and aerosols, viral load tended to be low.” After remarking on this jaw-dropping information, Ingram cites the closing statement for this study “The major limitation of our study was the large proportion of participants with undetectable viral shedding in exhaled breath for each of the viruses studied. We could have increased the sampling duration beyond 30 min to increase the viral shedding being captured…” and remarks that they go on to state that perhaps forced coughing migh thave helped. [Note: to review this study, see item #10 listed under toggle on this page titled, “What studies/literature reviews does CDC LIST to support its GUIDELINES for universal masking? Are they hoping nobody actually reads them?”]
Ingram refers back again to this last study stating, “So the issue, as it’s explained in this study, is that non-coughing or sneezing people are, by and large, not shedding virus in their ordinary breath.“
She remarks on how this relates to the (now blown) theory of asymptomatic shedding of virus, noting how this study had a hard time – under LAB CONDITIONS – detecting much of anything with actively infected (fever, active symptoms, etc.) and coughing individuals.
Last but not least, she notes that this concern (asymptomatic transmission) has been the entire premise upon which mask mandates have been predicated…!
STUDY: A cluster randomised trial of cloth masks compared with medical masks in healthcare workers (4/22/15)
Read study — National Center for Biotechnology Information, U.S. National Library of Medicine (NCBI)
Cliff Notes & Pull Quotes:
“This study is the first RCT of cloth masks, and the results caution against the use of cloth masks. This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection. Further research is needed to inform the widespread use of cloth masks globally. However, as a precautionary measure, cloth masks should not be recommended for HCWs, particularly in high-risk situations, and guidelines need to be updated.”
“In the interest of providing safe, low-cost options in low income countries, there is scope for research into more effectively designed cloth masks, but until such research is carried out, cloth masks should not be recommended. We also recommend that infection control guidelines be updated about cloth mask use to protect the occupational health and safety of HCWs.”
STUDY: Headaches and the N95 face-mask amongst healthcare providers (2006)
Cliff Notes & Pull Quotes:
This study sought “to determine the prevalence of headaches from the use of mask amongst healthcare workers in our institution.”
About 1/3 of respondents reported headaches with wearing N95 mask and this study identified “preexisting headaches and prolonged duration of N95 face-mask wear as important risk factors for the development of these headaches.”
Results showed lower blood oxygenation (hypoxia) and/or increased blood C02 (hypercapnia) can cause people required to wear masks all day to have painful headaches.
Conclusion: “This study highlights the relatively high prevalence of headaches with the use of the N95 face-mask amongst healthcare workers working in high-risk areas. Shorter duration of face-mask wear may reduce the frequency and severity of these headaches. Further studies should be performed to confirm this observation and elucidate the mechanisms underlying this association.”
STUDY: Preliminary report on surgical mask induced deoxygenation during major surgery (4/19/08)
Read study — National Center for Biotechnology Information (NCBI)
Cliff Notes & Pull Quotes:
“Results: Our study revealed a decrease in the oxygen saturation of arterial pulsations (SpO2) and a slight increase in pulse rates compared to preoperative values in all surgeon groups. The decrease was more prominent in the surgeons aged over 35.
Conclusions: Considering our findings, pulse rates of the surgeon’s increase and SpO2 decrease after the first hour. This early change in SpO2 may be either due to the facial mask or the operational stress. Since a very small decrease in saturation at this level, reflects a large decrease in PaO2, our findings may have a clinical value for the health workers and the surgeons.”

STUDY: Surgical masks as source of bacterial contamination during operative procedures (6/27/18)
Cliff Notes & Pull Quotes:
This study evaluated bacterial shedding on surgical masks.
“Results: The bacterial count on the surface of SMs increased with extended operating times; significant difference was found between the 4- to 6-hour and 0-hour groups (p < 0.05). When we analysed the bacterial counts from the same surgeon, a significant increase was noted in the 2-hours group. Moreover, the bacterial counts were significantly higher among the surgeons than the OR. Additionally, the bacterial count of the external surface of the second mask was significantly higher than that of the first one.”
“Conclusions: The source of bacterial contamination in SMs was the body surface of the surgeons rather than the OR environment. Moreover, we recommend that surgeons should change the mask after each operation, especially those beyond 2 hours. Double-layered SMs or those with excellent filtration function may also be a better alternative.”
CDC Policy Review: Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures (05/2020)
Cliff Notes & Pull Quotes:
This article reviews: “the evidence base for personal protective measures and environmental hygiene measures, and specifically the evidence for the effectiveness of these measures in reducing transmission of laboratory-confirmed influenza in the community” and discusses, “the implications of the evidence base for inclusion of these measures in pandemic plans.”
Findings include:
1) “although mechanistic studies support the potential effect of hand hygiene or face masks, evidence from 14 randomized controlled trials of these measures did not support a substantial effect on transmission of laboratory-confirmed influenza. We similarly found limited evidence on the effectiveness of improved hygiene and environmental cleaning”
2) “In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks…”
3) “Proper use of face masks is essential because improper use might increase the risk for transmission…”
4) “We did not find evidence that surgical-type face masks are effective in reducing laboratory-confirmed influenza transmission, either when worn by infected persons (source control) or by persons in the general community to reduce their susceptibility…“
NEWS: Public Health Experts Keep Changing Their Guidance on Whether or Not to Wear Face Masks for Coronavirus (3/3/2020)
Cliff Notes & Pull Quotes:
In March, CDC was “specifically not recommending [masks] for healthy people trying to protect against COVID-19.” This article provides scientific basis for why masks are ineffective:
1) “It seems kind of intuitively obvious that if you put something—whether it’s a scarf or a mask—in front of your nose and mouth, that will filter out some of these viruses that are floating around out there,” says Dr. William Schaffner, professor of medicine in the division of infectious diseases at Vanderbilt University. The only problem: that’s not likely to be effective against respiratory illnesses like the flu and COVID-19. If it were, “the CDC would have recommended it years ago,” he says. “It doesn’t, because it makes science-based recommendations.”
2) The science, according to the CDC, says that surgical masks won’t stop the wearer from inhaling small airborne particles[this link added for additional reference], which can cause infection.
3) The CDC also does not recommend N95 respirators…“Seriously people- STOP BUYING MASKS!” tweeted Dr. Jerome Adams, the U.S. Surgeon General, on Feb. 29. “They are NOT effective in preventing general public from catching #Coronavirus…In an interview with Fox & Friends, Adams said that wearing a mask can even increase your risk of getting the virus. “Folks who don’t know how to wear them properly tend to touch their faces a lot and actually can increase the spread of coronavirus.” [this link added for additional reference]
4) Other reasons [people may turn to wearing masks] are purely psychological…“By using a mask, even if it doesn’t do a lot, it moves the locus of control to you, away from the virus. It gives the individual a greater sense of control in this otherwise not-controlled situation…Lynn Bufka, a clinical psychologist and senior director for practice, research and policy at the American Psychological Association, suspects that people are clinging to masks for the same reason they knock on wood or avoid walking under ladders. “Even if experts are saying it’s really not going to make a difference, a little [part of] people’s brains is thinking, well, it’s not going to hurt. Maybe it’ll cut my risk just a little bit, so it’s worth it to wear a mask,” she says.”
5) “Seeing people around you wearing masks when you’re not can also heighten anxiety about coronavirus and make it seem like the virus is nearby and spreading, even if it’s not, Bufka says.”
STUDY: Effect of face veil on ventilator function among Saudi adult females (1/1/12)
Read study — Pakistan Journal of Medicinal Studies Online
Cliff Notes & Pull Quotes:
“Objective: The use of face veil called “niqab” by women to cover their faces at public places is a common practice in some Muslim communities. The long-term effect of niqab use on ventilatory function (VF) has not previously been reported. The aim of this cross-sectional study was to compare VF between niqab wearing and non-niqab wearing healthy Saudi females….Forced vital capacity (FVC), forced expiratory volume in one second (FEV1), FEV1/FVC (%), and maximal voluntary ventilation (MVV) were recorded using a digital spirometer. Results: Mean values of FVC, FEV1, FEV1/FVC (%) and MVV for niqab wearers were significantly lower than the corresponding values for non-niqab wearers. Significant negative correlation was found between the FVC and FEV1 values and the number of hours of the use of face veil per day. Conclusions: Long-term use of traditional niqab use can affect VF.”
“In conclusion, our data show that there are differences in VF tests among niqab and non-niqab wearing Saudi adult females, where values for niqab users are lower than the values for those who do not use niqab… “
STUDY: Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial (2009)
Read Study — Jacobs, J. L. et al. (2009) “Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial,” American Journal of Infection Control, Volume 37, Issue 5, 417 – 419.
Cliff Notes & Pull Quotes:
This study is directly referenced as part of the white paper, “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” as follows: “N95-masked health-care workers (HCW) were significantly more likely to experience headaches. Face mask use in HCW was not demonstrated to provide benefit in terms of cold symptoms or getting colds.”
RE: all studies/medical reviews cited and discussed in “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” the following general conclusion is drawn (in addition to otherwise going into many aspects worth reading):
“Conclusion Regarding That Masks Do Not Work
No RCT study with verified outcome shows a benefit for HCW or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions.
Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
Masks and respirators do not work.”
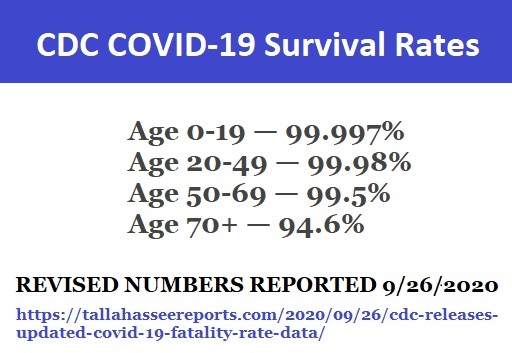
VIDEO: CDC MASK DECEPTION (5/27/2020)
Cliff Notes & Pull Quotes:
Peggy Hall (The Healthy American) pokes sizeable holes in the “studies” presented by the CDC and which serve as the basis for their guideline on universal masking of healthy people.
“This is the guideline that every state board of health and every local board of health is following. These are the guidelines from the CDC that businesses are following – that schools are going to be following…I am going to show you right now how corrupt and fraudulent this information is. These CDC individuals must think that you are ignorant. They must think that you are not going to dig deeper. Either that or they are ignorant, they are incompetent, or they are intentionally deceiving you with the information.”
She takes us to the CDC’s website and navigates to the “cloth face covers” section. Re: this terminology, she states, “they are changing the language so that is doesn’t sound so nefarious,” and goes on to compare this terminology with that of “masks” and why it is significant. She then moves on to a video of the U.S. Surgeon General instructing citizens on how to make a mask from materials found around the house (like an old scarf). She continues, “…so, someone wants to take care of themselves, they want to protect themselves – they go to the CDC because their state board of health told them to – because their governor recommended that they do that – because their neighbor said so – because the media said so – because the local board of health said so. Maybe the board of supervisors are giving these guidelines and the links go back to the CDC. Anytime you find these links to the CDC, you need to dig deeper. So let’s dig deeper.”
She then reviews the examples of “recent studies” presented on the CDC’s website. There are seven of them listed at the time of this video. She states, “Well, look at this – of course we should wear a mask made of an old scarf – because look at it – this looks really impressive!” Then she notes that first, there is no link (and you can see that no studies presented have links). Before moving on to take an in-depth look at each example, she asks us to focus on the science and to contemplate the fact that this is what the health orders are based on.
Ultimely, this review raises serious questions, reasonably demands science as the basis for policy and emphasizes our role as citizens, in requiring explanation of that science from leaders in all sectors.
STUDY: N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial (2019)
Read Study — “N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial,” JAMA. 2019; 322(9): 824–833.
Cliff Notes & Pull Quotes:
This study is directly referenced as part of the white paper, “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” as follows: “Among 2862 randomized participants, 2371 completed the study and accounted for 5180 HCW-seasons. … Among outpatient health care personnel, N95 respirators vs medical masks as worn by participants in this trial resulted in no significant difference in the incidence of laboratory-confirmed influenza.”
RE: all studies/medical reviews cited and discussed in “Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy,” the following general conclusion is drawn (in addition to otherwise going into many aspects worth reading):
“Conclusion Regarding That Masks Do Not Work
No RCT study with verified outcome shows a benefit for HCW or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions.
Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
Masks and respirators do not work.”
STUDY: Findings from a household randomized controlled trial of hand washing and face masks to reduce influenza transmission in Bangkok, Thailand (2/17/11)
Read study — National Center for Biotechnology Information (NCBI)
Cliff Notes & Pull Quotes:
Findings: Influenza transmission was not reduced by interventions to promote hand washing and face mask use.
News Coverage & Commentaries…

ATTORNEY LEIGH DUNDAS EXPLAINS WHY IT'S DANGEROUS TO WEAR MASKS (2022)
Transcript (with bold text for emphasis):
Hey guys, attorney Leigh Dundas here, you know before I did human rights work I did a lot of representation of environmental companies, big Fortune 100 / 500 companies that were suing each other so I do have some background in math and science. And today I wanted to talk to you about the mandatory mask wearing and oxygenation levels in the body. A lot of our big cities and counties and school districts and churches and box stores have said, you know what – you have to wear a mask.
A couple of things to note folks, if you’re wearing a mask and thinking that it actually stops the spread of the virus, that’s actually pretty much not true in most contexts because the mesh of the mask is too big and the virus particle just slips right on through. The second thing that we know about masks – and this is really the most important thing – is they do impede the flow of oxygen into your system.
So, recently, a county down here in Southern California decided that they were going to put a mandatory mask order in place. And the residents said, show us your science that says it’s safe for us to wear masks all the time. And they couldn’t really show the science. So, a lot of the residents, while the county was debating the issue this last week, went on the steps of County Hall, put a pulse ox meter on their finger – if you’re not familiar with this device, it’s a little device that just clamps on the end of your finger and it measures the amount of oxygen in your system. And, when the people put it on before they had the mask in place, they had about 98 – 99 percent oxygenation which is pretty standard and that’s very normal. Every single person, within a few minutes of putting a mask on their face, dropped to 92% or below, which is hypoxic range. The average range at which participants found themselves was 86%. It is worth noting that Medicare and your insurance company will actually pay for you to get supplemental oxygen if you are below 88%. And the average of our participants was two points below that. Two of the people dropped into the 70s, which is severe hypoxia land where cardiac arrest and organ failure and death can occur. One of those was a very fit nurse – she dropped into 76% zone. And the other one was a runner. She runs every day and she was at 79%.
So, a lot of times, people say well so and so said to do it – it must be safe. You know, our government told us that DDT was safe. They told us Agent Orange was safe. They told us that pregnant women should smoke Camel’s, and that was safe. And it wasn’t safe, folks. In the same way that a lot of that stuff wasn’t safe, this is not safe. If you’re walking around with a mask on your face and your oxygen level is down in the red zone – that is not okay.
So, a lot of cities and schools, though, and counties – they weren’t really getting the point. So what we did was we made a reenactment of something that actually happened in China. A few weeks ago, if you didn’t hear, two teenage Chinese boys who were at school and had to have a mask on died while they were wearing the mask. We didn’t want that to happen here. We made a reenactment, here in America, that people could track with and understand, and we released that simulation last night online. Immediately, within the first two hours, I was getting dozens and dozens of people saying, I had to wear a mask and something bad happened. One of the worst stories that I heard was from an aunt whose nephew went into the hospital. They put him in pre-op – he was about to have surgery – they put a mask on him while he was in pre-op – and his oxygen rate dropped to 80 to 87% – the hospital could not get it north of 87%. Finally, the mother ripped a mask off his face and, within two breaths, his oxygen was back at 97%. Another woman said that her friends a hairdresser here in Southern California and ended up passing out on the job and hitting her head on the chair on the way down.
So, a couple of things to note – there is a federal agency responsible for ensuring workplace safety, including the right amount of oxygen in the stores that people are working in – It’s called OSHA. And what it has to say, if you go to their website right now, about missing oxygen – oxygen that’s going subpar, below the level it should be at – is it will cause the person to experience “increased breathing rate, accelerated heart rate, impaired thinking and coordination – even in people who are resting faulty judgment, exhaustion, nausea, vomiting, loss of consciousness , convulsions and cardiac standstill.” For those of you not familiar with that last term, let me break it down for you: your cardiac is your heart unit. If it’s in a standstill, you’re gonna die. Last quote from OSHA, “even if a worker survives the hypoxic insult, his organs may show evidence of hypoxic damage which may be irreversible.”
For all of you folks who are tired of feeling bad when you’re out in a mask, Go out and buy yourself one of these (shows a pulse oximeter), And the next time you’re out and you’re feeling bad, put it on your finger. Maybe you’re just having a bad day and that’s why you’re feeling bad. Or maybe your oxygen is in the red zone and you need to do something to fix it. I’m not giving you medical or legal advice, I’m just telling you what I would do. I would sit down in that store. I would report it to my boss. I would report it to corporate. If I didn’t work there I would report it to the store manager. And then I would report it to OSHA and the media. And if I were feeling really poorly, I’m going to dial 911 because I don’t want to die of a heart attack.
Final note on this point guys – and I am speaking right now to that hospital who put a kid in a mask and kept his oxygen rate in the ’80s – And I’m talking to the city of Irvine in the city of Costa Mesa and every single county in our state that still has a mandatory mask order – and LA unified school district That wants every student and teacher in a mask this fall – and our state department of education and every damn box store – quit drinking the frickin Kool-Aid. You have got zero science to show this is safe. All of the science shows the exact opposite. I’m going to make it really simple: you cannot afford this liability. Because the next time some employee or parishioner or student or customer goes down on your premises and cracks their head wide open on your concrete floor, every single attorney in a 30 mile radius is going to be begging to nail your ass to the wall for a 7-digit verdict through settlement. And rightly so.
We need to start reinserting some sanity into these decisions.
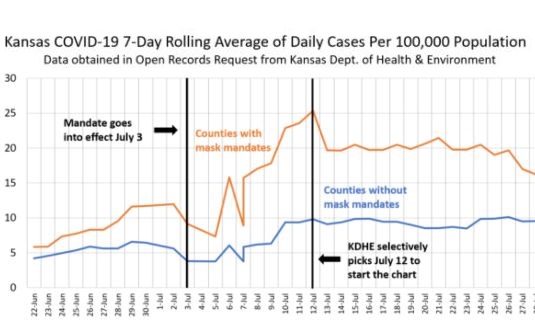
NEWS: Kansas Department of Health and Environment Hid Data to Justify Mask Mandate - spoiler: counties without mandates had lower infection rates! (8/13/2020)
Cliff Notes & Pull Quotes:
Kansas health department tried to manipulate official statistics and presentation of data in order to hide the fact that 90 counties without mask mandates demonstrated LOWER coronavirus infection rates than 15 counties with mandates.
NEWS: Texas COVID Cases Drop to Record Low Nearly Three Weeks After Mask Mandate Lifted (3/29/2021)
Newsweek feature citing record low cases of Coronavirus in Texas since state lifted mask mandated and reopened businesses.
Positive test rate now 4.95% (lowest since start of pandemic) and hospitalizations at a 6 month low.
The seven-day moving average number of cases has dropped to “lowest level since mid-June.”
On March 2, 2021, Governor Abbot declared, “Texas is OPEN 100%” and noted, “I also ended the statewide mask mandate.” The state was reopened effective March 10. 2021.
Also noted: the state of Mississippi also removed its restrictions around the same time as Texas and has also seen a drop in virus cases and hospitalizations.
MANDATE RESULTS IN GERMANY: N95s Make No Difference (3/1/2021)
Twitter post makes reference to the following chart with commentary:
“Germany: Bavaria made N95/FFP2 masks mandatory (e.g. shops and public transports) from January, 18th. Other states in Germany didn’t. 6 weeks later: N95 masks make no difference, the curves are absolutely identical.” [emphasis added]
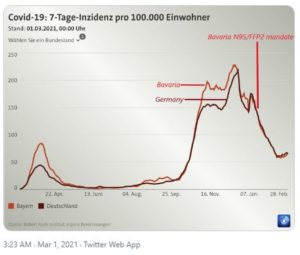
EMPLOYER "MUST READ" -- EDITORIAL: Human factors expert: masks may increase business liability (6/30/2020)
Cliff Notes & Pull Quotes:
This article is the first in a two-part series. The second article addresses potential for cognitive impairment and other risks from CO2 build-up in face masks.
This article features expert commentary from Sal Fariello, retired expert witness “who has written engineering reports for lawyers and insurance companies dealing with accident causation, human injury biomechanics, human factors, safety and warnings, and product failures.”
Fariello shares concern re: unintended consequences of mask mandate that “businesses may be subject to liability lawsuits if patrons or employees are injured in accidents that could be caused by carbon dioxide (CO2) build-up under masks.”
Highlights of his commentary:
1) Universally applied mandates don’t consider “…people respond differently to intoxicating substances…physical size, health status, age, and other medications can cause people to react to the same amounts of alcohol differently…same applies to medications: dosages are often tied to body weight…it would be incorrect to conclude that elevated levels of CO2 are “safe” for all people.”
2) A lot of evidence counters CDC’s assertion that “carbon dioxide, indeed, will collect between the mask and face but not in dangerous amounts and certainly not enough to cause hypercapnia.”
3) S. Navy Diving Manual refers to hypercapnia as “abnormally high level of carbon dioxide in the blood and body tissues” and “lists confusion, inability to concentrate, and headache among the symptoms and warns that “hypercapnia may give the diver little or no warning prior to onset of unconsciousness.”
4) Many articles discuss possible hazards re: CO2 under masks. Some have justified disregarding these by looking only “ at worst-case scenarios (i.e., levels required to cause unconsciousness) when dismissing concerns about CO2.”
5) In talking to cashiers at local retailers, Fariello states: “I spoke to cashiers at Publix and Walgreens today, and they both told me the same horror story, that every employee in the store was sick from the masks, suffering from brutal headaches, dizziness, and exhaustion.”
6) He claims one experiencing these while wearing a mask “is likely suffering from other symptoms of hypercapnia, even if they’re not aware of them.”
Discussion on hypercapnia:
1) One can have high CO2 even if oxygen level is normal “Because these effects are so vague, you might not realize that they are caused by hypercapnia.”
2) NIH states CO2 exposure can cause: headaches, inability to concentrate, vertigo, double vision, suffocation by air displacement, incapacitation and unconsciousness, tinnitus and seizures.
3) One review of debate on CO2 toxicity cites conflicting opinions – one university professor claims CO2 can only cause harm in high concentration while Dr. Amesh Adalja (Johns Hopkins Center for Health Security) contradicts, stating, “Someone wearing an N95 mask for a prolonged period of time may have alterations in their blood chemistry.”Critical point made — they are talking “about different things: toxicity versus impairment,” noting, “alcohol toxicity occurs around 0.45% blood alcohol concentration (BAC), but impairment starts as low as 0.05%.” Also, while a law cites .08% BAC, drivers may/may not be impaired at that level; police perform sobriety tests to determine impairment regardless because it can occur “well below level of toxicity.”
4) Decision-making and problem resolution are among cognitive performance items impacted by even “short-term CO2 exposure” (beginning at 1,000 ppm) and while other countries have 1,000 ppm limit, U.S. limit set by OSHA is 5,000 ppm over 8 hours.
5) This review determined, “Findings suggest that there is a direct effect of low-level exposure to CO2 on performance,” which “may profoundly affect job competence and learning ability.”
6) Exact details are provided associating CO2 levels and symptoms including dry throat, tiredness, dizziness, heart rate variability, peripheral blood circulation, headache, eye irritation, upper respiratory symptoms, decreased cognitive ability and critical response, immune problems that “can cause diffuse inflammatory vascular injury,” fatigue and lower performance, etc.
Additional Commentary:
1) Related cognitive concerns prompted newer cars to be equipped with internal CO2 monitors.
2) Innate and adaptive immune responses are suppressed when elevated CO2 lowers blood PH and this degradation “can begin with just 30 minutes of exposure and can last up to 3 days after CO2 is returned to normal levels.”
3) Some excuse claims like those above insisting most wear masks for short stints outside home. However, many employees wear masks “for 6-10 hours at a time, and complaints of headaches are common, indicating that the masks are causing some sort of physiological changes.”
4) Masks can reduce oxygen to lungs says Stanford engineer, “N95 masks are estimated to reduce oxygen intake by anywhere from 5 to 20 percent. That’s significant, even for a healthy person.”
5) OSHA requires “air breathed by employees must have an oxygen content of at least 19.5 percent.” Below this level can cause “increased breathing rates, accelerated heartbeat, and impaired thinking or coordination.”
6) Masks trap exhaled gases and reduce oxygen level of air being breathed in again.
Conclusion:
Fariello suggests performing studies measuring actual CO2 and O2 concentrations under variety of masks and determining how much time is required “for blood concentrations to recover if they are indeed affected by wearing masks.”
He also cautions masks worn by employees for hours on end or older people for short periods could cause “lapses in judgment or impairment of motor skills that could lead to falls or to car accidents.
He concludes, “If businesses require masks, they should be aware of their potential liability if accidents occur on their premises or shortly after leaving their premises.”

NEWS: No Spike in Florida Coronavirus Cases Despite Lack of Enforceable Mask Mandate (10/9/2020)
Cliff Notes & Pull Quotes:
On 9/25/2020, Florida’s Gov. Ron DeSantis “took a major step, lifting key coronavirus restrictions at the state level” that included removing enforcement of mask mandates across the state. Over more than two weeks now, Florida has recorded “no spike in cases of the Chinese coronavirus.
Despite businesses (restaurants) now allowed to operate at full capacity, “the state of the coronavirus in Florida has remained relatively unchanged…” [additional supporting statistics are cited]
Deaths have continued to decline over this same period and hospital capacity showed plentiful hospital bed availability, with 23.47 percent available statewide.” [additional supporting statistics are cited]
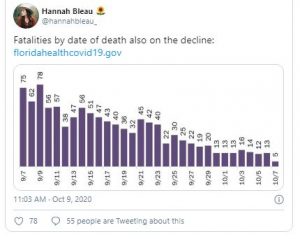
The article discusses opposition from some local leaders, in spite of the above outcomes and in particular regard to “removing the penalty for mask mandates.” Note, local authorities are able to keep their ordinances in this respect however, they are prevented from enforcement (penalties have effectively been removed).
Last month, DeSantis declared, “We will never do any of these lockdowns again, and I hear people say they’ll shut down the country, and honestly I cringe.”
The article discusses the fact that some officials continue to cite CDC’s recommendations and that there have been a number of conflicting opinions about masks (efficacy, universal masking, etc.) and noted that , in July, CDC director, Dr. Robert R. Redfield stated 1-2 months of universal masking “could bring the Wuhan virus ‘under control.;”
Also, in discussing the conflicting opinions, this feature notes several examples of leaders who have demonstrated a conflict between what they say and what they do as relates to advocating for universal masking. Specifically, “…Fauci is among several leaders who have been spotted in public places without masks. The list includes New York Gov. Andrew Cuomo (D), as well as Democrat presidential hopeful Joe Biden (D), both of whom have passionately pressed for the widespread use of masks…” [article includes numerous photos of these individuals in public without masks]
The article closes by noting that a recent study adds to “mounting controversy over the effectiveness of universal masking, revealing that some face coverings, such as neck gaiters, are actually worse than going maskless…” and that “Biden has suggested that he would implement a nationwide mask mandate as president, although he has flip-flopped in recent weeks and admitted that such a move may not be constitutionally sound.”
EDITORIAL: Horowitz: Exposing the maskerade: The questions every American should be asking about indefinite mask mandates (7/24/2020)
Cliff Notes & Pull Quotes:
An all-encompassing feature raising key questions about face mask efficacy and demanding scientific answers. Pointed, logical and factual.
Opening: “The trope of “just shut up and wear a mask” is not science, ordered liberty, or constitutional governance. It’s what they do in North Korea. We need real debate on the effectiveness of masks, the type of masks, the situations in which they are worn, the duration of time, the benchmarks that need to be met to measure effectiveness, and the process for promulgating these rules. We are no longer 24 hours into an emergency. We are four months into this virus, and it’s time to function like the representative republic that we are. There are numerous political and scientific questions any thinking person should be asking at this point:…”
Body: points made and questions raised are too good to paraphrase – very worth reading…
Conclusion: “And these people have the nerve to call conservatives anti-science? The question we must ask ourselves is this: if our government can now mandate such a personal and disruptive lifestyle change to our bodies with assertions that contradict their own long-standing evidence from just weeks ago and with so many unanswered questions, what else can they do to us without presenting evidence or a transparent and democratic debate? It appears that “my body, my choice” only applies to murdering babies. We deserve hearings and we deserve answers. We are citizens, not subjects. Just because this virus came from China doesn’t mean the politicians can use it as a pretext to turn us into China.”
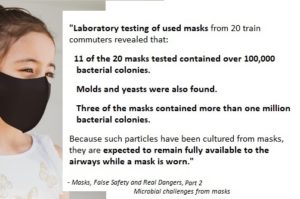
NEWS: 7 Long-Term Side Effects of Wearing Face Masks (6/11/2020)
Note: because the original link to this MSN feature appears to have suddenly gone MIA, we searched internet archives for a link you can use to view it, as it originally appeared on MSN’s website, on 6/11/2020. (also, we happened upon a video that someone put together, as well…).
Pull Quotes:
“1. Shortness of Breath and Lightheadedness
“Activities that result in the expulsion of air, such as talking, yelling, singing and exercising can result in the accumulation of carbon dioxide between the face and the mask,” says Dr. Lili Barsky. “These symptoms are seen due to increases in CO2 levels in your body,” says Dr. Rashmi Byakodi. “Breathing over exhaled air that turns into carbon dioxide might make you feel dizzy.”
- Headaches
“Long term wearing of masks can result in prolonged and repeated episodes of headaches,” says Dr. Byakodi. “Headaches may occur due to the band fitting around the head all day, stress from breathing through the mask, or slight changes in oxygen and carbon dioxide levels in the blood,” says Dr. Leann Poston.
- Acne
“Re-wearing unwashed reusable masks or re-wearing disposable masks can lead to inhalation of dust, pollen, bacteria and other particle contaminants trapped within the mask material,” says Dr. Barsky. This can clog your pores and cause breakouts, primarily around your chin.
- Development of Chronic Dermatitis
“In the case of surgical masks, the nonwoven fabric is made by using chemicals to bond the fibers together. Some people who have sensitive skin can break out and develop some form of dermatitis as a result of the repeated exposure,” says Dr. Sanul Corrielus. “This can have long term consequences in terms of recurrence and scarring of the skin around the face.”
- A Weakened Immune System
“There are studies indicating that low oxygen levels in the tissues (hypoxia) can suppress some aspects of the immune response,” says Dr. Esteban Kosak. “Scientific investigations have proven that a prolonged denial of enough oxygen in the body can cripple the ability of our immune system to tackle infections which is even worse with older and younger people.”
- Skin Wrinkles
According to Viseslav Tonkovic-Capin, MD, Dermatologist and Editor at DermBoard, another effect of long term face mask use is: “new patterns of skin wrinkling.” It’s best to stock up on some lotions and facial moisturizers.
- Development of Chronic Respiratory Conditions
“In the case of the surgical masks which are made of nonwoven fabric, the exposure for some people can trigger an asthma-like inflammatory response in the lungs,” says Dr. Corrielus. “This is likely due to the inhalation of the microfibers in the material that forms the masks.”
- How to Not Get Sick From Your Face Mask
“It is advised to take regular breaks to breathe fresh air,” says Dr. Byakodi. “The impact of wearing a mask depends on your health, any pre-existing respiratory illnesses, the type of mask, and the extent of time the person wears it.” To wear your face mask correctly, do as the CDC advises:
“Wash your hands before putting on your face covering
Put it over your nose and mouth and secure it under your chin
Try to fit it snugly against the sides of your face
Make sure you can breathe easily.”
And to get through this pandemic at your healthiest, don’t miss these Things You Should Never Do During the Coronavirus Pandemic.”
EDITORIAL: Horowitz: E-MASK-ulation: How we have been lied to so dramatically about masks -- What did the scientific literature say before the issue became political? (9/10/2020)
Cliff Notes & Pull Quotes:
A few important items to note before providing the skinny on this article:
This feature was published just ahead of this Twitter post noting the CDC warning that ordinary (non-N95) masks will do nothing to protect you against wildfire smoke because “they do not catch small particles.” As user, Alex Berenson, responded, “Fun fact: smoke particles are far larger than SARSCoV2. Your mask protects…well, no one.”
This feature was published on the same day that Dr. Fauci clarified that virus transmission is not limited to via “droplets” [that don’t go too far before falling to the ground when one coughs, etc.] but via aerosol particles [that cannot be stopped by such masks, as has been noted across many studies, features and commentaries – some listed on this website – and the above-referenced warning containing CDC’s own inadvertant admission].
And here’s
warning ordinary (non-N95) masks will do nothing to protect you against wildfire smoke because “they do not catch small particles.” Fun fact: smoke particles are far larger than #SARSCoV2. Your mask protects… well, no one.

NEWS: Dentists say 'mask mouth' can cause serious health complications, including strokes (8/7/2020)
Pull Quotes:
“They said dental problems associated with “mask mouth,” including gum disease, could lead to serious complications.”
“Gum disease — or periodontal disease — will eventually lead to strokes and an increased risk of heart attacks…”
“We’re seeing inflammation in people’s gums that have been healthy forever, and cavities in people who have never had them before,” Ramondi said. “About 50% of our patients are being impacted by this, [so] we decided to name it ‘mask mouth’ — after ‘meth mouth.’”
“People tend to breathe through their mouth instead of through their nose while wearing a mask,” Sclafani said. “The mouth breathing is causing the dry mouth, which leads to a decrease in saliva — and saliva is what fights the bacteria and cleanses your teeth.”
EMPLOYER "MUST READ": Research does not support face mask orders (7/1/2020)
Cliff Notes & Pull Quotes:
This article is the second in a two-part series. The first article addresses potential for cognitive impairment and other risks from CO2 build-up in face masks.
Opens with county charter and asserts, “County commissioners have not made a case for the necessity of mask wearing by the general public, and they can’t, because there is little evidence showing that such a policy prevents transmission of COVID-19.”
Next cites WHO and its conflicting statements, noting, “…there is very little evidence that there is much to gain [by wearing masks], and there is more to lose than mask advocates care to admit” and, “Despite the WHO’s new position on encouraging face masks, the June 5 guidelines state:
- “There is limited evidence that wearing a medical mask by healthy individuals in households… or among attendees of mass gatherings may be beneficial as a measure preventing transmission.”
- “cluster randomized controlled trials… showed no impact on risk of laboratory-confirmed influenza.”
- “There is no direct evidence (from studies on COVID-19 and in healthy people in the community) on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19.”
- “At the present time, the widespread use of masks by healthy people in the community setting is not yet supported by high quality or direct scientific evidence and there are potential benefits and harms to consider.
Notes statement by WHO Director, “Masks can also create a false sense of security…I cannot say this clearly enough: Masks alone will not protect you from COVID-19.”
Focuses next on science, which ultimately serves to demonstrate masks are not effective, despite arguments by proponents of universal masking. A few notes worth mention re: science:
1) proponents argue masks are intended to stop spread, not protect wearer; assert if 50-80% of population wear them, spread will be reduced by (only) 8.4%. However, this could not be verified and “…studies cited by Vox, which they claim show benefits of mask wearing, are based on models that assume masks work…”
2) Studies by Cambridge are cited while feature notes, “…Cambridge authors admit they “make assumptions and simplifications about the effectiveness of facemasks…” and that effectiveness number is based on bacterial studies, which are irrelevant since “the largest virus is smaller than the smallest bacterium…”
3) Other materials speculate / argue for masks on the basis that they would “theoretically be most useful in stopping aerosols” yet this article points out, “…actual tests of cloth face masks show they allow between 74% and 90% penetration by aerosols.”
4) While mask mandates should be based on science, they are mostly based on “mathematical models” that, by the several examples provided (examples that serve as basis for most federal and state response) have proven wildly inaccurate.
5) Medical reviews of studies demonstrate inefficacy of wearing masks to slow spread. Medical professor, Paul Hunter, reviewed 31 such studies and determined, “Randomized-controlled trials are supposed to trump observational studies… and randomized-controlled trials have all been pretty much negative on face masks in the community.”
6) Denis Rancourt performed thorough review of randomized controlled studies and concluded, “… all show that masks and respirators do not work to prevent respiratory influenza-like illnesses.” He noted a) “N95-masked healthcare workers were significantly more likely to experience headaches” and b) “Masks do not prevent transmission of influenza virus by health-care workers or community members in households” and c) “None of the 17 studies reviewed established a conclusive relationship between mask/respirator use and protection against influenza infection” and d) “No statistically-significant protective effect of masks or respirators against respiratory infection was found” and e) “no study exists that shows a benefit from a broad policy to wear masks in public.”
7) Two doctors featured in Center For Infectious Disease Research and Policy do not recommend masks for general public as “there is no scientific evidence they are effective in reducing the risk of SARS-CoV-2 transmission” and argue against efficacy of masks re: transmission in China and cloth masks, in particular.
8) Even if believed effective, masks become saturated with moisture in about 20 minutes, rendering them less effective barriers against viruses. Public Health Director for Quebec “said masks work for medical professionals because they follow strict guidelines for taking them on and off and discard them after each use.”
9) Widespread confusion re: different types of masks is also a problem. N95 respirators are designed to protect wearer and those with exhalation valves have NO filtering so are totally ineffective.
10) OSHA “Guidance on Preparing Workplaces for COVID-19 (OSHA 3990-03 2020) lists masks and other PPE as the “least effective protection measure” and ads for facemasks in UK have been banned “because they’re “misleading, irresponsible and scaremongering.”
11) National health services that do NOT recommend masks include Danish Health Authority (“…Furthermore, mouth or face masks can cause more harm than good.”), Finish Institute for Health and Welfare (“…no evidence…extensive use of masks by healthy people will help reduce infections.”), Norwegian Institute of Public Health (“…no scientific basis for recommending…”), Public Health Agency of Sweden (“…not needed in everyday life.”) and UK National Health Service (recommends only for public transport or hospital visitation).
12) Wearing surgical face masks in surgical settings has never been shown to decrease post-op infection – instead, a 50% decrease was reported after OMITTING face masks.
Article returns to opening point, “Little to lose” or “significant unforeseen harm?” by:
1) Citing UK Telegraph March news report, “There is no reliable scientific evidence to suggest [face masks] work at scale and experts…worry they may cause significant unforeseen harm.”
2) Citing consequences including impaired thinking or coordination, weakened immune systems, increased spread of viruses, and increased liability for businesses
3) Reminding readers of a separate article re: “confusion, headaches, and suppression of the immune system due to build-up of CO2 inside the mask (hypercapnia).
4) Noting A) Dr. Fauci called attention to habits that can increase spread of viruses (60 Minutes) B) Denis Rancourt’s review underscores “potential harms” including potential increased transmission C) Dr. Russell Blaylock’s warning, “by wearing a mask, the exhaled viruses will not be able to escape and will concentrate in the nasal passages, enter the olfactory nerves, and travel into the brain.”
5) Noting all of the above present liability concerns for employers: “CDC Guidance, employees are supposed to wash their hands ‘after putting on, touching, or removing cloth face coverings.’ That means they must wash their hands every time they touch the mask. Each masked employee represents a potential fine or lawsuit if they are seen touching their face mask.“
6) Noting OSHA Guidance on required proper maintenance/disposal of masks and that used masks are considered “biomedical waste”
7) Citing Florida Administrative Code Rule 64E-16.002, raising other liability questions (“Are companies that offer masks to customers or employees also responsible for the proper disposal of those masks? Are they ensuring proper decontamination of employee masks that get reused or proper storage before cleaning?”). Citing another law, the feature notes, “Just because the government encourages or requires masks, employers are not protected from the liabilities that come with them.“
8) Arguing for removal of mask mandates on legal grounds and on behalf of liability to business community —- noting research does not support claims that masks are effective in limiting the spread of COVID-19 it asserts that it cannot be argued that ineffective measures are “necessary to eliminate or contain conditions that threaten the health, safety, or welfare of the citizens of the county,” as is required by the County Charter, so the emergency order that mandates masks should be revoked, and it would be best to do so before a business is sued for one of the many downsides of forcing all their employees and customers to wear masks.
EDITORIAL: Horowitz: From Fort Benning to Japan and Hawaii, face masks are not working (8/3/2020)
Cliff Notes & Pull Quotes:
The author notes, “Even following protocols in the military didn’t stop the coronavirus from spreading. One will not find a greater degree of compliance to a mask mandate than with one placed on military trainees by drill sergeants. That’s why, if masks are really the viral placebo their devoted cult worshipers make them out to be, one would expect mask mandates to work wonders in these environments. Except, they didn’t work – just like they didn’t work in Japan, Hawaii, Israel, California, Miami, or any other place where they’ve shown near universal compliance for months, yet the virus spread rapidly.”
He then details the Fort Benning outbreak noting its stopped at the 22% threshold. He draws comparisons from there before stating, ” The working theory is that most people have some degree of cross-immunity from other coronavirus colds and that the virus does not transmit homogenously from every infected individual.”
Then he observes, “On the one hand, nothing seems to prevent a spread in the population, but on the other hand, a de facto herd immunity threshold is hit around 20%. The quicker we achieve this through the younger population, the more we will see results like we’ve witnessed in the military.”
Next, he speaks to current events in Japan and makes subsequent comparisons to states here in the US: “They are now panicking in Hong Kong with cases surging despite a universal mask mandate in place for months. Countries like Japan and Hong Kong are as disciplined and as clean as they come. But you can’t stop a pandemic flu. Thankfully, there really is no reason to panic because the rate of serious cases is even less in Asia thanks to their inherent partial immunity….The same holds true for a state like California, which had the earliest stay-at-home order in March and has never exited a modified phase one reopening. We all know how that has turned out. The same holds true for Israel and Australia. In fact, in the ultimate irony, the only countries that seem to remain flat are the Nordic countries, which have aggressively resisted the idea of public masking.”
Finally, he concludes, “What we are seeing over and over again is that in areas where the virus already spread, the lockdowns don’t work at all. In areas where there was a low rate of seroprevalence at the time of the lockdown, they successfully delay the spread temporarily. But because those policies are unsustainable until eradication, which could take years, they are actually forestalling herd immunity, keeping vulnerable people at risk longer, crushing their society and economies, and ensuring that so many seniors die of isolation and atrophy.”
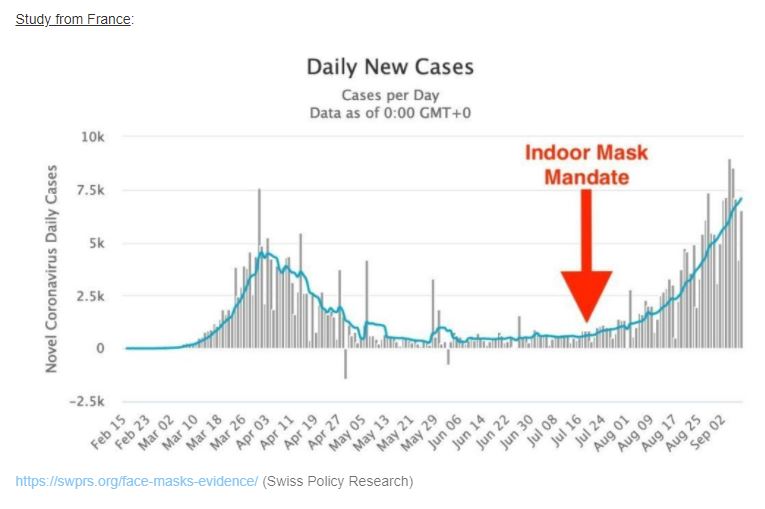
EDITORIAL: Mayor: Health Officials Justify Mask Mandates For Political Reasons, Not Science (8/5/2020)
Pull Quotes:
“As a public official sworn to support and defend the Constitution of the United States which, above all, was instituted to protect the individual rights of those who elected me, this is frightening. If public officials are being given only the information I was provided during this meeting and do not conduct their own research, citizens will have personal choices taken from them in the name of social conditioning, not proven scientific data.
When public officials concentrate their resources more on forwarding an agenda than championing individual rights and liberties, our republic is lost.”
NEWS: Nashville Democrat Mayor’s Office Accused Of ‘Fabricating’ Coronavirus Numbers To Hide LOW Numbers Tied To Bars, Restaurants (9/17/2020)
Cliff Notes:
This story that went nationwide underscores the concern of politically-driven mandates (as opposed to scientific ones), particularly given the fact that it was due to low transmission in local bars and restuarants that numbers were alledgedly fudged.
Note, in bars and restuarants, masks are not worn to the extent of other stores and locations throughout this county that has had a mandate in place for months. It begs the question, shouldn’t there be even more transmission if masks work and/or the virus is that highly contageous?
Pull Quotes:
“The coronavirus cases on lower Broadway may have been so low that the mayor’s office and the metro health department decided to keep it secret…”
“The discussion involves the low number of coronavirus cases emerging from bars and restaurants and how to handle that and most disturbingly how to keep it from the public…”
“Health department official Leslie Waller asked senior adviser Benjamin Eagles: “This isn’t going to be publicly released, right? Just info for Mayor’s Office?” Eagles responded: “Correct, not for public consumption.”
“They are fabricating information. They’ve blown their entire credibility,” Glover claimed. “It’s gone, I don’t trust a thing they say going forward …nothing…We raised taxes 34 percent and put hundreds, literally thousands of people out of work that are now worried about losing their homes, their apartments, etc, and we did it on bogus data…that should be illegal!”
“Again, we weren’t told by the mayor’s office this wasn’t true. We were told to file a Freedom of Information Act request,” the local station concluded. “Which allows us now to ask the question: why are you keeping this from us? Why would you even want to? It’s just the real numbers and what could possibly be an honorable motive?”
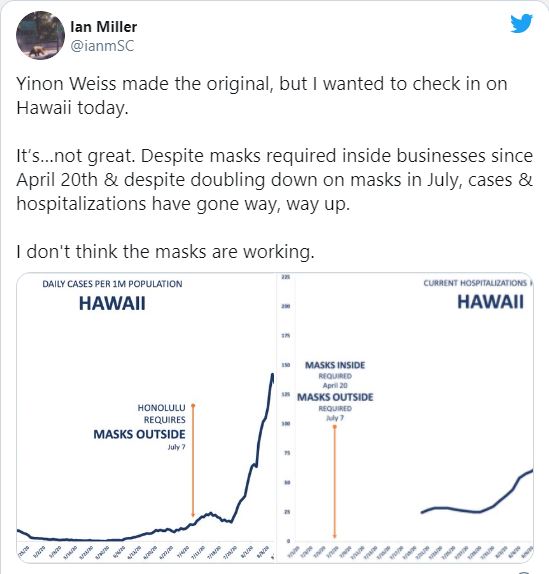
EDITORIAL: Horowitz: Coronavirus cases, hospitalizations soar in Hawaii since indoor and outdoor mask mandates (9/1/2020)
Cliff Notes & Pull Quotes:
Feature opens with question, “At what point do results and outcomes begin to matter?” Current policies continue without “debate, votes, benchmarks, or transparency” while madates in place for months show they are “worthless and that the virus spreads as it spreads, regardless of human input.”
Horowitz states Hawaii is latest example and notes:
1) no randomized controlled trials exist to show universal masking works to stop transmission of respiratory viruses
2) Like Philippines and Peru, Hawaii has maintained strict lockdown (since April) with indoor and outdoor mask mandates (since July), yet “results are the same as they have been in every place that tried to put up a cloth in front of the inexorable spread…”
3) Since mask mandates, case count grew more than tenfold in Hawaii. “If mask-wearing were as effective as the cult-like devotion to it claims…this result would be impossible.”
4) Hawaii is most isolated state, its tourism/commerce has been halted and “…Hawaiian Airlines has the strictest mask policies among all airlines.”
5) According to the New York Times, Hawaii has a high degree of compliance. The few people caught without masks have not only be cited, but arrested too. “Ditto for Peru, which had a universal mask mandate for months but has the most COVID-19 deaths per capita in the world.”
6) Reminds readers Dr. Fauci “said in July that there are no plans to conduct a randomized clinical trial to asses the effectiveness of universal mask-wearing in stopping the spread” and notes the “litmus test” providing these real world results in Hawaii are proof enough masks are not effective in stopping the spread.
7) If masks work, why does the CDC recommend one who comes into contact with an infected person for at least 15 minutes “…should quarantine, ‘irrespective of whether the person with COVID-19 or the contact was wearing a mask or whether the contact was wearing respiratory personal protective equipment (PPE)?”
8) Despite flimsy “science,” CDC’s director, Dr. Robert Redfield, stated, “If we could get everyone to wear a mask right now, I think in four, six, eight weeks, we could bring this epidemic under control.“
9) Horowitz notes, “Hawaiians were wearing masks for nearly 20 weeks in an island state before the virus spread much at all. Yet it still appeared with a vengeance in July.“
10) Reminds readers CDC cited results from 10 RCTs indicating, “no significant reduction in influenza transmission with the use of face masks.”
Horowitz concludes by pointing out, “Typically, in order to issue such a draconian and personal regulation of one’s person – to the extent that could ever be constitutional – the government must produce substantial evidence that the restriction is necessary and effective and propose its implementation through the least restrictive means for the minimal amount of time necessary…”
NEWS: Mask Fatigue: Some North Texas Workers Claim Headaches, Shortness Of Breath And Anxiety (7/29/2020)
Pull Quotes:
“McKINNEY, Texas (CBSDFW.COM) – The mask mandate to keep Texans from spreading COVID-19 is coming with some side effects.”
“Some people who are forced to wear face masks all day in the workplace complain of headaches, shortness of breath and anxiety.”
VIDEO - MEDICAL TESTIMONY: Group Suing Tulsa Leaders Over Mask Mandate (9/9/2020)
Pull Quote: “First Court Case to Challenge Masks! Tulsa Doctors sue to abandon masks. They allege masks don’t help the wearer or others, and they cause O2 deficiency, harming health. They claim irrefutable evidence. The Court’s decision in this matter will have far reaching implications.”
Transcript:
“…thank you very much, my name is Jim Meehan, I’m a medical doctor. I’m an opthamologist that specializes in occular inflammation and immunology. I’m a former medical editor that knows how to read the medical science. I read more than the top titles and the abstracts; I look at the methodologies. When I looked at the methodologies of the science being used to support community wearing of masks, I found a real posity [definition: smallness of number; fewness] of solid, high level science. In fact, we’ve been studying this issue for over thirty years with regards to the transmission of influenza in the population.
One of the reasons that we have never recommended the community wearing of medical masks is because it’s been shown at the highest levels of science; randomized controlled trials, meta analysis of randomized controlled trials, to not be effective; that hand washing, social distancing – masks add almost nothing to that equation. So it has a very marginal, at best, efficacy and those studies are in healthcare workers and hospital settings in which we have an optimal environment; with higher exchange, um, low temperatures — nothing like what our community is encountering.
Now, in general, I think we should always resist medical mandates. We don’t need lawmakers, um, intruding upon the medical decision-making that should be left between a patient and a doctor, after fully informed consent. They need to consider the risks, benefits and alternatives. And this issue of community wearing of medical masks – we have not done a fair risk analysis for the population. We have not informed them that the mask can block arterial oxygen – it can block oxygen intake significantly – that’s been demonstrated in experiments all over the world; it’s been studied in surgeons in an optimal environment, where there’s a higher level of oxygen in the operating suite – higher air exchange. I’ve worn a medical mask in surgical procedures over 10,000 times and I can tell you that they do induce physiological changes; um, I’ll start to develop a tremor after about thirty minutes of mask wear in that high air exchange, higher oxygen level, cool environment. Imagine what untrained members of our community are doing when they are wearing them in the Oklahoma summer…”
MEDICAL ARTICLE: Healthy People Should Not Wear Face Masks (6/12/2020)
Read medical article — Jim Meehan, M.D.
Cliff Notes & Pull Quotes:
A well-articulated overview with links to sources making the case for why healthy people should not wear face masks. One key point, for example, “Face masks decrease oxygen, increase carbon dioxide, and alter breathing in ways that increase susceptibility and severity of CoVID-19”
Asthma sufferers warned not to wear face masks amid coronavirus pandemic (5/20/2020)
Cliff Notes & Pull Quotes
The Daily Record reports asthma sufferers warned not to wear face masks as experts claim they “can make breathing harder for 12% of Brits.”
“…Asthma UK are advising people who suffer with the illness against covering up…The government has advised the people with respiratory conditions don’t need to wear face coverings – so if you are finding it hard, then don’t wear one.”
*NOTE — this and other features call attention to the potential for negative health impact of wearing masks by individuals with asthma and/or other conditions (like hypotension, COPD, etc.). Features like “Brain Hypoxia: Causes, Symptoms and Diagnosis” remind readers that, when suffering hypoxia, such individuals can be at greater risk for heart attack, stroke and/or irregular heartbeat.
NEWS: Two boys drop dead in China while wearing masks during gym class (5/6/2020)
Pull Quotes:
“Two Chinese boys dropped dead within a week of one another while wearing face masks during gym class, according to a report.”
“One of the teens was only minutes into his gym class when he fell backward…’He was wearing a mask while lapping the running track, then he suddenly fell backwards and hit his head on the ground,’ his father, who…said he believes that the mask his son was required to wear to school played a role in his death.”
“I don’t think mask-wearing has caused this sudden death,” Cao [Cao Lanxiu, professor at Shaanxi University of Chinese Medicine] said, though she added that it was impossible to say without an autopsy.”
“Six days after his death, the second student collapsed…He had been wearing an N95 respirator and running a 1,000-meter exam when the fatal incident occurred…Though it’s not known whether the masks played a role in either death, several schools in Tianjin and Shanghai have canceled physical education exams, according to the report.
REPORT: 13-year-old girl in Germany died suddenly - autopsy doesn't rule out CO2 intoxication (9/11/2020)
Read article (9/25/2020)
Read article (9/28/2020)
Cliff Notes & Pull Quotes:
On 9/11/2020, a 13-year old girl “suddenly collapsed and died” while wearing a protective mask for prolonged period of time. The autopsy has become a source of controversy now because it has not been concluded yet, not could it exclude CO2 intoxication or sudden cardiac arrest.
The first feature is a few short paragraphs followed by sections covering a variety of controversies sparked by this story. One section covers an expert’s description of how death can occur, “There are masks that have no medical purpose, but which harm people…Children cannot compensate for it when they breathe back too much CO2. They then start to develop a wrong respiratory drive and they do not notice when they are almost suffocating and there are disorders in the kidneys, the electrolytes and there are disorders of the heart rate. And then you just fall over and you’re dead.” Another section describes how a fact checker became “enraged about dissenting opinions” while another section shares warning from professional association of pediatricians about CO2 under masks.
The second feature is a few short paragraphs providing additional clarification about autoposy that has become a source of controversy.
NEWS: Europe's Top Health Officials Say Masks Aren't Helpful (8/7/2020)
PULL QUOTES:
“Denmark boasts one of the lowest COVID-19 death rates in the world. As of August 4, the Danes have suffered 616 COVID-19 deaths, according to figures from Johns Hopkins University. That’s less than one-third of the number of Danes who die from pneumonia or influenza in a given year…”
“All these countries recommending face masks haven’t made their decisions based on new studies,” said Henning Bundgaard, chief physician at Denmark’s Rigshospitale, according to Bloomberg News. Denmark is not alone…”
“Others, echoing statements similar to the U.S. Surgeon General from early March, said masks could make individuals sicker and exacerbate the spread of the virus. “Face masks in public places are not necessary, based on all the current evidence,” said Coen Berends, spokesman for the National Institute for Public Health and the Environment. “There is no benefit and there may even be negative impact.” In Sweden, where COVID-19 deaths have slowed to a crawl, public health officials say they see “no point” in requiring individuals to wear masks…”
“The problem with mask mandates is that public health officials are not merely recommending a precaution that may or may not be effective. They are using force to make people submit to a state order that could ultimately make individuals or entire populations sicker, according to world-leading public health officials. That is not just a violation of the Effectiveness Principle. It’s a violation of a basic personal freedom.”

Jogger's lung collapses after he ran for 2.5 miles while wearing a face mask (5/12/2020)
Cliff Notes & Pull Quotes:
After jogging 2.5 miles with a face mask, a 26-year-old Chinese man’s lung collapsed.
He became “breathless and started suffering severe chest pain” and his lung “which shrunk by 90 per cent, had collapsed and even edged his heart towards the right side of his chest.”
‘We see no point in wearing a face mask,’ Sweden’s top virus expert says as he touts the country’s improving COVID numbers (7/29/2020)
Pull Quotes:
“The Health Agency of Sweden says that since hitting a peak in late June, the infection rate has fallen sharply. That’s amid an increase in testing over the period. “The curves are going down and the curves for the seriously ill are beginning to approach zero,” Tegnell said.”
“Tegnell also broached the subject of face masks, which the World Health Organization recommends people use when social distancing isn’t possible. “With numbers diminishing very quickly in Sweden, we see no point in wearing a face mask in Sweden, not even on public transport,” he said.
Tegnell has consistently argued that Sweden’s approach is more sustainable than the sudden lockdowns imposed elsewhere. With the risk that Covid-19 might be around for years, he says completely shutting down society isn’t a long-term option. Meanwhile, many countries that thought they’d brought the virus under control are now seeing second waves. Tegnell called those developments “worrying.”
EDITORIAL: Disturbingly COVID Incurious (8/5/2020)
Cliff Notes & Pull Quotes:
Primary assertion: “In other words, COVID-19 no longer justifies mandatory mask-wearing, surveillance contact tracing (a protocol for containing community spread at onset, not months into it), closing schools, quarantining healthy people, shuttering economies, and abandoning our elders to suffer, despair, and die alone.”
Opening graph: “This pandemic is waning by all measures that count. Regardless, the public at large remains deeply frightened, submissive, compliant, and disturbingly incurious. Incurious about the onslaught of redundant, irrational, fact-starved messaging recited by “trusted voices,” be they government officials or mainstream-media propagandists. Incurious about the glaring absence of relevant details from technocratic health officials, such as start and end dates for reported cases and reported deaths. Incurious about what precisely is being tested and reported. Incurious about cumulative all-cause deaths over comparative historical time periods. Incurious about the much larger agenda driving the increasingly incoherent narrative rooted in emotional triggering headline after headline.
RE: the issue of masks, this feature states: “We’ve received numerous submissions of attempts to refute Dr. Denis Rancourt’s white paper we published in June, entitled “Masks Don’t Work.” (RCReader.com/y/mask). Due to space constraints, we are publishing these efforts online at RCReader.com/y/mask9. While any ad hominem attacks are unfortunate, efforts were robust whether successful or not. Please read for yourself. Finally, we are not anti-mask. We are against using the force of government to mandate a healthy population potentially harming themselves with inappropriate masking, based on unproven, unscientific rationale and agendas that do not serve the people’s best interests. Finally, mask wearing has a benefit that deserves mention. Wearing masks can give the wearer a sense of control in circumstances that are out of his/her control. That is no small thing. Efficacy or not, if wearing a mask provides a sense of security, and of protection for oneself and others, then that is a choice worth making. It is a choice, and by its very nature, must remain so to preserve the spirit of the perceived benefit.”
Note, this feature presents a long list of sources in support its content, with links to each source.
EDITORIAL: Making face masks mandatory is not backed by science or law (7/25/2020)
Cliff Notes & Pull Quotes:
Author, John Carpay, is an attorney and president of the Justice Centre for Constitutional Freedoms.
His argument in opposition to the mandating of universal masking focuses on the fact that, while many doctors/public health offocials support such, it doesn’t maen the science is settled. He points to studies, organizations (like the WHO) and medical organizations and professionals (including Dr. Fauci) that raise health concerns, a false sense of security and the lack of direct evidence that wearing masks this way stops respiratory virus from spreading.
He notes, “A WHO guideline from June 5, 2020 states: “At present, there is no direct evidence (from studies on COVID-19 and in healthy people in the community) on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19. … At the present time, the widespread use of masks by healthy people in the community setting is not yet supported by high quality or direct scientific evidence and there are potential benefits and harms to consider.”
He raises other concerns about potential liabilities of universal masking that include impairment of communication, violation of personal autonomy and human dignity, impact of identity loss (dehumanization factor), etc.
He concludes this feature stating, “What is “unprecedented” in 2020 is not COVID but a new social and political experiment of locking up an entire population of millions of healthy people, pushing many of them into unemployment, poverty, depression and loneliness, all of which significantly reduce overall health….Another “unprecedented” feature of 2020 is politicians and chief medical officers who ignore settled medical opinion that the best way to vanquish a virus (and to protect the vulnerable from it) is to allow it to spread amongst people who are younger, stronger and healthier. Once “population immunity” (“herd immunity”) is established, the virus cannot easily spread further, and therefore has far less chance of harming the vulnerable. If wearing a mask truly works to reduce the spread of a virus, then mask-wearing will hurt the vulnerable by delaying the acquisition of population immunity. Settled medical opinion about herd immunity cannot simply be disregarded or dismissed. Those who believe that we can and should try to stop the spread of a virus amongst healthy and invulnerable people must prove and justify their novel approach.”
Lawyer John Carpay is president of the Justice Centre for Constitutional Freedoms.
VIDEO: Heather Mac Donald & Dennis Prager on Mask-Wearing 9/2/2020
Cliff Notes & Pull Quotes:
Transcripted segments between Heather Mac Donald (HM) and Dennis Prager (DP) include:
HM: “The state is using our bodies – is inscribing its power on our bodies – the way the pre-modern state did with torture to convey its message. We become the message of the state which says, “Be afraid. Be very afraid.” There is no outdoor transmission. Period. Infection requires close contact in a confined indoor space.
DP: “For a prolonged period and very close to one another. Ten to thirty minutes with one person who is talking right into your face, for that period of time, indoors. And then you might get the infection.”
HM: “That’s it. 15 minutes. The CDC contact tracing guidelines isn’t even interested in you unless you’ve been in 15 minutes of prolonged contact. These fleeting encounters outdoors with circulating air – viral dose matters. Fresh air absolutely makes it impossible to contract the virus and yet, this message – we say, “wear masks in public” – it is, it is conveniently ambiguous.”
DP mentions he can get fined $400 the first time in Glendale, CA [for not wearing mask in public] and that he will pay that, “rather than succomb to becoming a walking billboard of institutionalized fear because I follow the science, whereas Glendale doesn’t.”
HM: “That’s absolutely right and I actually think that the conservatives have made a mistake in resting their opposition to outdoor mask wearing on sheer libertarian values. If there were strong evidence of strong infection possibility outdoors, I think that there are legitimate grounds for the state power for the common good. So I’ll reluctantly wear masks indoors, but I’m not gonna do it outdoors.”
DP: “Well, I will tell you, a couple of weeks ago I spoke in Chicago and I had a meet and greet beforehand and I must have shaken hands and, on occasion, hugged about 50 strangers and – uh, maskless – and I am totally at peace with that and, in part, because I take hydroxychloroquine every week, with zinc…”
HM: “Well, I just got back from a conference in Vail, at the Steamboat Institute – same thing – it never – it doesn’t even occur to me – I think, even with this fake, phony “second wave,” the risk to any individual is still minute, given the size of this country, the number of cases, the number of deaths we’ve had is still a minute fraction of anything else that Americans put up with – I
NEWS: Driver in crash may have passed out from wearing N95 mask too long (4/25/2020)
Pull Quotes:
“”The crash is believed to have resulted from the driver wearing an N95 mask for several hours and subsequently passing out behind the wheel due to insufficient oxygen intake/excessive carbon dioxide intake,” the post read in part.”
“…While we don’t know this with 100% certainty, we do know that the driver had been wearing an N95 mask inside the vehicle for several hours and ultimately passed out while operating the vehicle.”
“‘All this being said, It is certainly possible that some other medical reason could’ve contributed to the driver passing out. We are not trying to cause public alarm or suggest wearing an N95 mask is unsafe. The original point of the post was to state that in most cases, the wearing of this type of mask while operating a vehicle with no other occupants is unnecessary,’ the police wrote.”